

Phosphorylated Myosin Light Chain 2 (p-MLC2) as a Molecular Marker of Antemortem Coronary Artery Spasm
- PMID: 27643564
- PMCID: PMC5031170
- DOI: 10.12659/msm.900152
Phosphorylated Myosin Light Chain 2 (p-MLC2) as a Molecular Marker of Antemortem Coronary Artery Spasm
Abstract
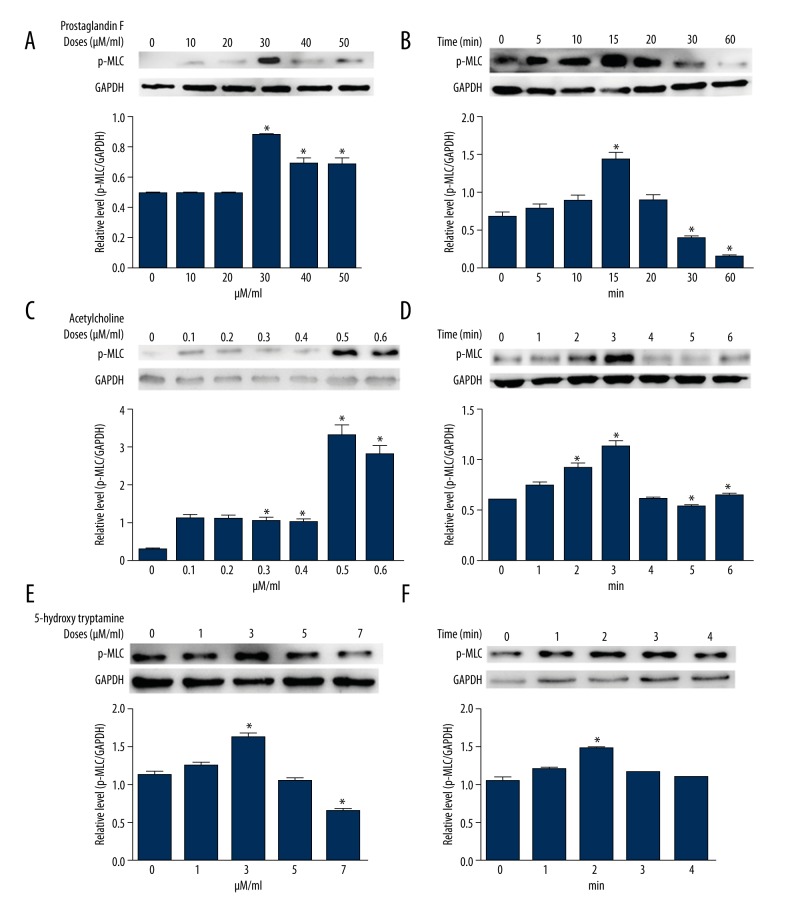
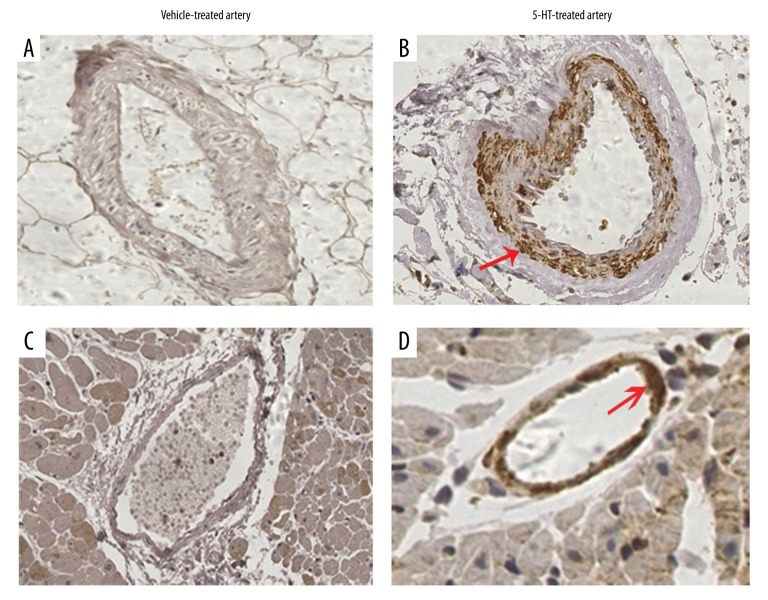
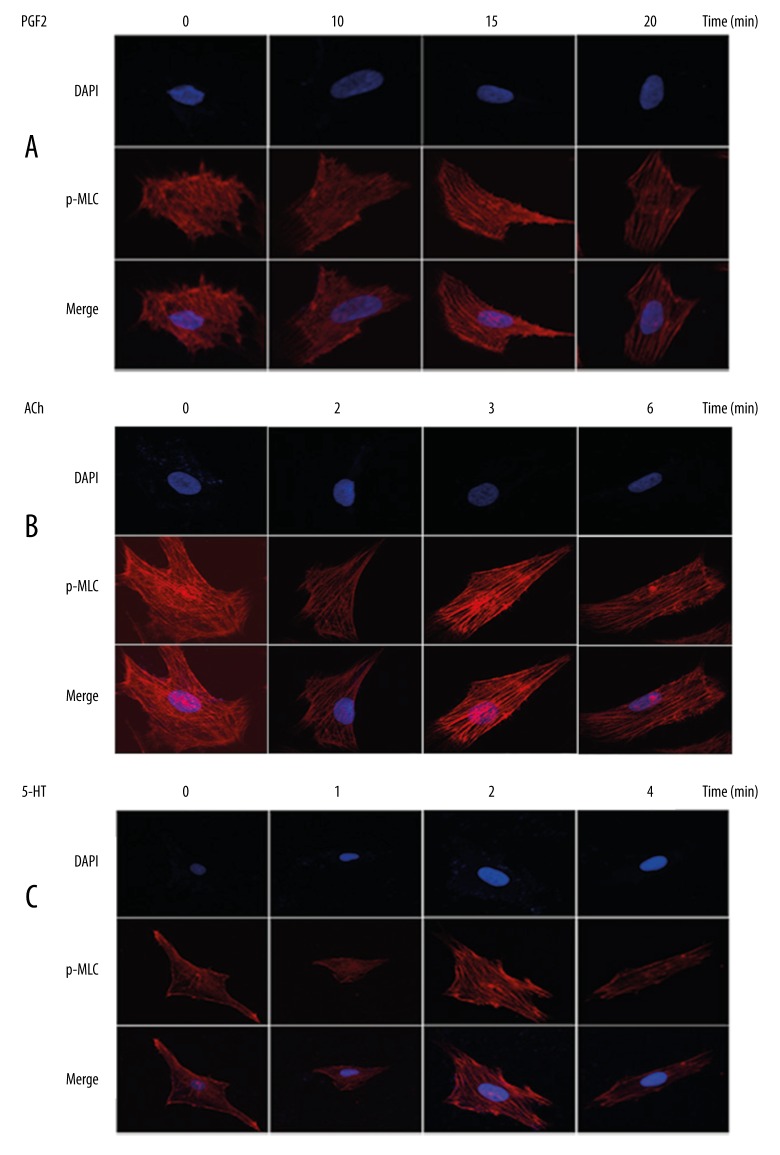
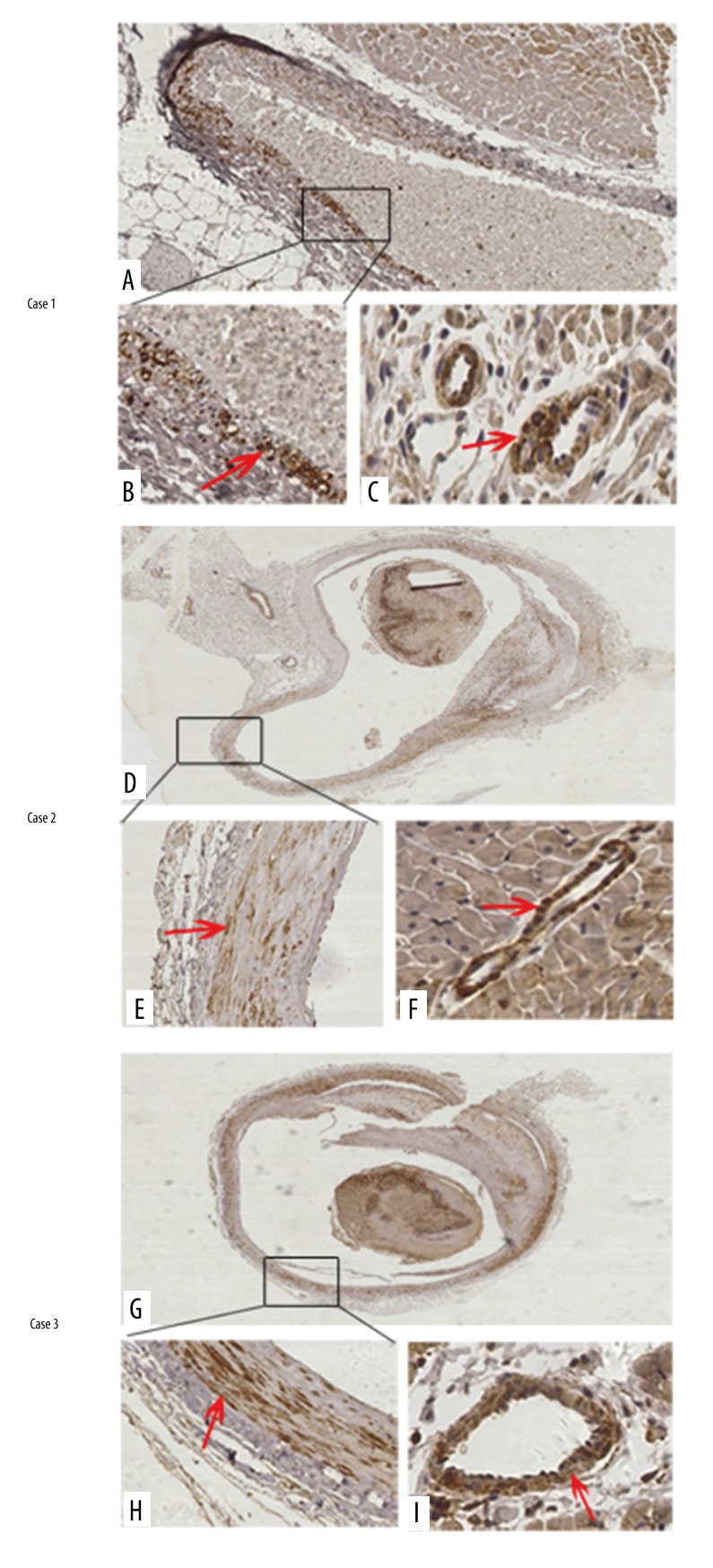
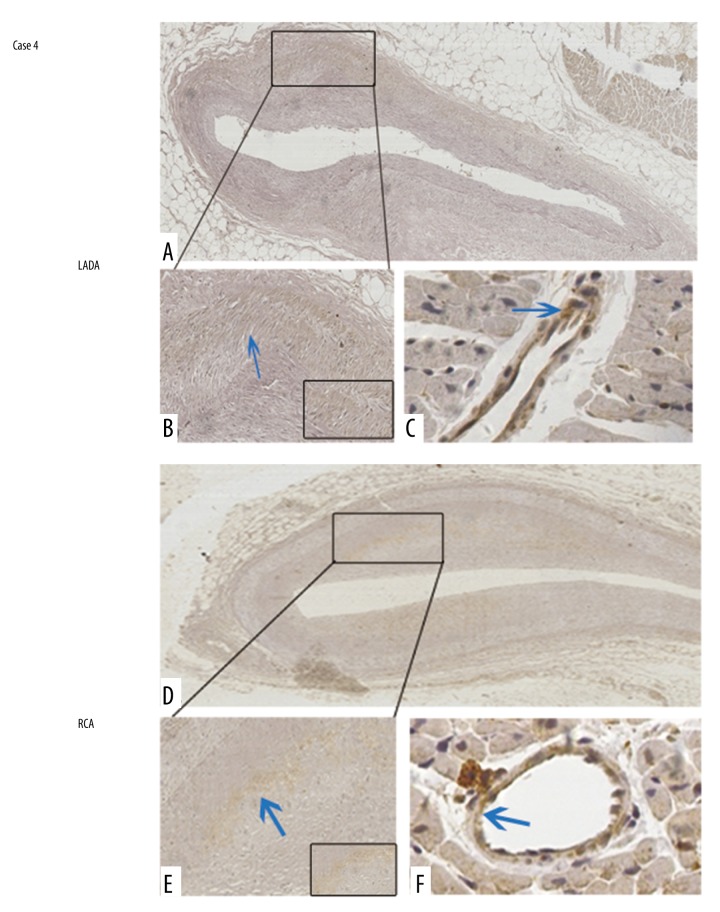
BACKGROUND It is not uncommon that only mild coronary artery stenosis is grossly revealed after a system autopsy. While coronary artery spasm (CAS) is the suspected mechanism of these deaths, no specific biomarker has been identified to suggest antemortem CAS. MATERIAL AND METHODS To evaluate the potential of using phosphorylated myosin light chain 2 (p-MLC2) as a diagnostic marker of antemortem CAS, human vascular smooth muscle cells (VSMCs) were cultured and treated with common vasoconstrictors, including prostaglandins F2α (PGF2α), acetylcholine (ACh), and 5-hydroxy tryptamine (5-HT). The p-MLC2 level was examined in the cultured cells using Western blot analysis and in a rat model of spasm provocation tests using immunohistochemistry (IHC). Effects of increased p-MLC2 level on VSMCs contractile activities were assessed in vitro using confocal immunofluorescence assay. Four fatal cases with known antemortem CAS were collected and subject to p-MLC2 detection. RESULTS The p-MLC2 was significantly increased in VSMCs after treatments with vasoconstrictors and in the spasm provocation tests. Myofilament was well-organized and densely stained in VSMCs with high p-MLC2 level, but disarrayed in VSMCs with low p-MLC2 level. Three of the 4 autopsied cases showed strongly positive staining of p-MLC2 at the stenosed coronary segment and the adjacent interstitial small arteries. The fourth case was autopsied at the 6th day after death and showed negative-to-mild positive staining of p-MLC2. CONCLUSIONS p-MLC2 might be a useful marker for diagnosis of antemortem CAS. Autopsy should be performed as soon as possible to collect coronary arteries for detection of p-MLC2.
Figures
Similar articles
-
Phosphorylated CPI-17 and MLC2 as Biomarkers of Coronary Artery Spasm-Induced Sudden Cardiac Death.Int J Mol Sci. 2024 Mar 3;25(5):2941. doi: 10.3390/ijms25052941. Int J Mol Sci. 2024. PMID: 38474189 Free PMC article.
-
SIRT1-mediated deacetylation of NF-κB inhibits the MLCK/MLC2 pathway and the expression of ET-1, thus alleviating the development of coronary artery spasm.Am J Physiol Heart Circ Physiol. 2021 Jan 1;320(1):H458-H468. doi: 10.1152/ajpheart.00366.2020. Epub 2020 Oct 23. Am J Physiol Heart Circ Physiol. 2021. PMID: 33095054
-
Aberrant endoplasmic reticulum stress mediates coronary artery spasm through regulating MLCK/MLC2 pathway.Exp Cell Res. 2018 Feb 15;363(2):321-331. doi: 10.1016/j.yexcr.2018.01.032. Epub 2018 Jan 31. Exp Cell Res. 2018. PMID: 29378169
-
[Research Progress and Forensic Application on the Pathogenesis of Coronary Artery Spasm].Fa Yi Xue Za Zhi. 2018 Feb;34(1):60-66. doi: 10.3969/j.issn.1004-5619.2018.01.012. Epub 2018 Feb 25. Fa Yi Xue Za Zhi. 2018. PMID: 29577707 Review. Chinese.
-
The Biochemical Markers Associated with the Occurrence of Coronary Spasm.Biomed Res Int. 2019 Sep 17;2019:4834202. doi: 10.1155/2019/4834202. eCollection 2019. Biomed Res Int. 2019. PMID: 31637257 Free PMC article. Review.
Cited by
-
Phosphorylated CPI-17 and MLC2 as Biomarkers of Coronary Artery Spasm-Induced Sudden Cardiac Death.Int J Mol Sci. 2024 Mar 3;25(5):2941. doi: 10.3390/ijms25052941. Int J Mol Sci. 2024. PMID: 38474189 Free PMC article.
-
O-GlcNAcylation: The Underestimated Emerging Regulators of Skeletal Muscle Physiology.Cells. 2022 May 30;11(11):1789. doi: 10.3390/cells11111789. Cells. 2022. PMID: 35681484 Free PMC article. Review.
-
Assessing Serum Levels of ADAMTS1 and ADAMTS4 as New Biomarkers for Patients with Type A Acute Aortic Dissection.Med Sci Monit. 2017 Aug 13;23:3913-3922. doi: 10.12659/msm.905092. Med Sci Monit. 2017. PMID: 28803253 Free PMC article.
-
Novel Insights Into DLAT's Role in Alzheimer's Disease-Related Copper Toxicity Through Microglial Exosome Dynamics.CNS Neurosci Ther. 2024 Oct;30(10):e70064. doi: 10.1111/cns.70064. CNS Neurosci Ther. 2024. PMID: 39428563 Free PMC article.
-
Unveiling the Molecular Mechanisms of Rosacea: Insights From Transcriptomics and In Vitro Experiments.J Cosmet Dermatol. 2025 Jan;24(1):e16753. doi: 10.1111/jocd.16753. J Cosmet Dermatol. 2025. PMID: 39823143 Free PMC article.
References
-
- Mortensen ES, Rognurn TO, Straume B, Jorgensen L. Evidence at autopsy of spasm in the distal right coronary artery in persons with coronary heart disease dying suddenly. Cardiovasc Pathol. 2007;16:336–43. - PubMed
-
- Basso C, Burke M, Fornes P, et al. Guidelines for autopsy investigation of sudden cardiac death. Virchows Archiv. 2008;452:11–18. - PubMed
-
- Wang HY, Yao QS, Zhu SH, et al. The autopsy study of 553 cases of sudden cardiac death in Chinese adults. Heart Vessels. 2014;29:486–95. - PubMed
-
- Maseri A, Labbate A, Baroldi G, et al. Coronary vasospasm as a possible cause of myocardial-infarction – conclusion derived from study of preinfarction angina. New Engl J Med. 1978;299:1271–77. - PubMed
-
- Buxton AE, Goldberg S, Harken A, et al. Coronary-artery spasm immediately after myocardial revascularization – recognition and management. New Engl J Med. 1981;304:1249–53. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
