

A dedicated neonatal brain imaging system
- PMID: 27643791
- PMCID: PMC5516134
- DOI: 10.1002/mrm.26462
A dedicated neonatal brain imaging system
Abstract
Purpose: The goal of the Developing Human Connectome Project is to acquire MRI in 1000 neonates to create a dynamic map of human brain connectivity during early development. High-quality imaging in this cohort without sedation presents a number of technical and practical challenges.
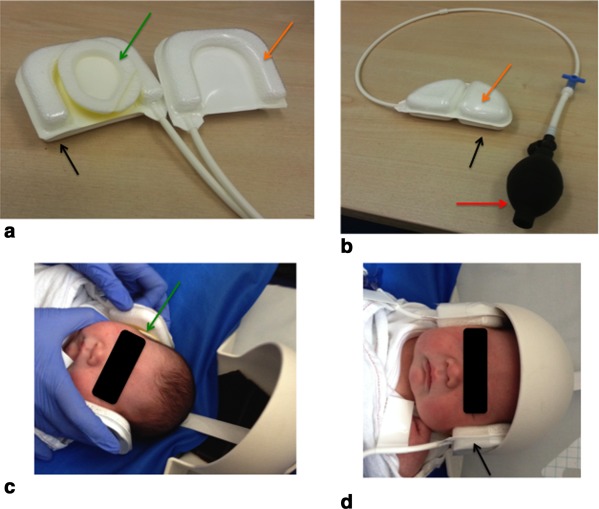
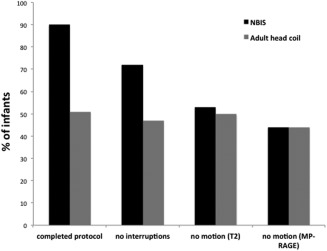
Methods: We designed a neonatal brain imaging system (NBIS) consisting of a dedicated 32-channel receive array coil and a positioning device that allows placement of the infant's head deep into the coil for maximum signal-to-noise ratio (SNR). Disturbance to the infant was minimized by using an MRI-compatible trolley to prepare and transport the infant and by employing a slow ramp-up and continuation of gradient noise during scanning. Scan repeats were minimized by using a restart capability for diffusion MRI and retrospective motion correction. We measured the 1) SNR gain, 2) number of infants with a completed scan protocol, and 3) number of anatomical images with no motion artifact using NBIS compared with using an adult 32-channel head coil.
Results: The NBIS has 2.4 times the SNR of the adult coil and 90% protocol completion rate.
Conclusion: The NBIS allows advanced neonatal brain imaging techniques to be employed in neonatal brain imaging with high protocol completion rates. Magn Reson Med 78:794-804, 2017. © 2016 The Authors Magnetic Resonance in Medicine published by Wiley Periodicals, Inc. on behalf of International Society for Magnetic Resonance in Medicine. This is an open access article under the terms of the Creative Commons Attribution-NonCommercial-NoDerivs License, which permits use and distribution in any medium, provided the original work is properly cited, the use is non-commercial and no modifications or adaptations are made.
Keywords: brain; head coil; neonatal; unsedated.
© 2016 The Authors Magnetic Resonance in Medicine published by Wiley Periodicals, Inc. on behalf of International Society for Magnetic Resonance in Medicine.
Figures





References
-
- Mathur AM, Neil JJ, McKinstry RC, Inder TE. Transport, monitoring, and successful brain MR imaging in unsedated neonates. Pediatr Radiol 2008;38:260–264. - PubMed
-
- Ureta‐Velasco N, Martinez‐de Aragon A, Moral‐Pumarega MT, Nunez‐Enamorado N, Bergon‐Sendin E, Pallas‐Alonso CR. Magnetic resonance imaging without sedation in neonates [in Spanish]. An Pediatr (Barc) 2015;82:354–359. - PubMed
-
- Golan A, Marco R, Raz H, Shany E. Imaging in the newborn: infant immobilizer obviates the need for anesthesia. Isr Med Assoc J 2011;13:663–665. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
