

Impact of an Analgesia-Based Sedation Protocol on Mechanically Ventilated Patients in a Medical Intensive Care Unit
- PMID: 27644010
- PMCID: PMC5237378
- DOI: 10.1213/ANE.0000000000001393
Impact of an Analgesia-Based Sedation Protocol on Mechanically Ventilated Patients in a Medical Intensive Care Unit
Abstract
Background: Recent attention to adverse effects of intensive care unit (ICU) sedation has led to the use of strategies that target a "lighter" depth of sedation. Among these strategies are "analgosedation" protocols, which prioritize pain management and preferentially use IV opioids before administration of continuously infused sedatives such as propofol or midazolam. We hypothesized that using an analgosedation protocol would result in a shorter duration of mechanical ventilation than a protocol with greater emphasis on IV sedatives
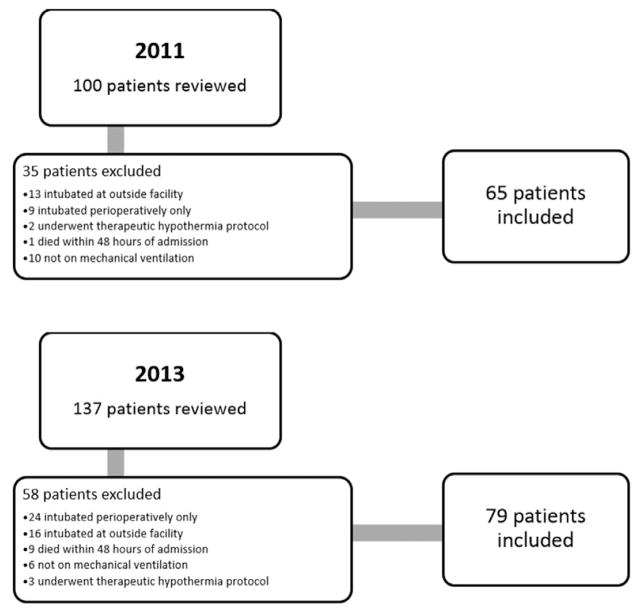
Methods: : We conducted a retrospective study comparing the duration of mechanical ventilation before and after implementation of an analgosedation protocol in a 24-bed medical ICU. Patients were aged 18 years or older and required mechanical ventilation where a light level of sedation was clinically appropriate. Exclusion criteria included a clinical need for deeper levels of sedation or tracheal intubation confined to the perioperative period.
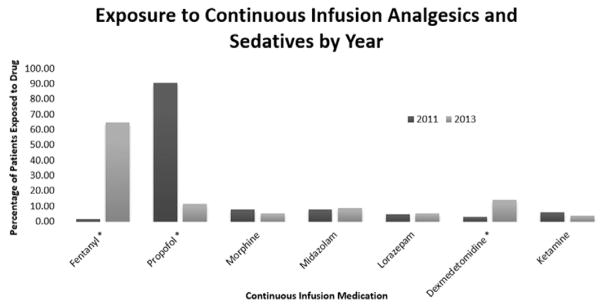
Results: Seventy-nine patients were included in the postimplementation group and 65 in the preimplementation group. After adjustment for baseline covariates, introduction of the 2013 analgosedation protocol was associated with a decreased duration of mechanical ventilation (-26.62 hours; 95% confidence interval, - 44.98 to -8.26, P = 0.005). Patients managed with the analgosedation protocol experienced a lighter level of sedation (median Richmond Agitation-Sedation Scale, -2.57 vs -1.25, P = 0.001) and improved pain management (median Critical-Care Pain Observation Tool score, 2.0 vs 1.5, P = 0.03). The use of continuously infused sedatives was reduced by 54.3% (92.3% vs 38.0%, P < 0.001).
Conclusions: Our findings suggest that implementation of an analgosedation protocol was associated with an overall lighter level of sedation, shorter mean ventilator duration, and a reduced use of continuous infusion sedatives. Further studies are needed to assess the impact of such protocols on ICU delirium.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Barr J, Fraser GL, Puntillo K, Ely EW, Gélinas C, Dasta JF, Davidson JE, Devlin JW, Kress JP, Joffe AM, Coursin DB, Herr DL, Tung A, Robinson BR, Fontaine DK, Ramsay MA, Riker RR, Sessler CN, Pun B, Skrobik Y, Jaeschke R American College of Critical Care Medicine. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41:263–306. - PubMed
-
- Skrobik Y, Ahern S, Leblanc M, Marquis F, Awissi DK, Kavanagh BP. Protocolized intensive care unit management of analgesia, sedation, and delirium improves analgesia and subsyndromal delirium rates. Anesth Analg. 2010;111:451–63. - PubMed
-
- Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med. 2014;370:444–54. - PubMed
-
- Devabhakthuni S, Armahizer MJ, Dasta JF, Kane-Gill SL. Analgosedation: a paradigm shift in intensive care unit sedation practice. Ann Pharmacother. 2012;46:530–40. - PubMed
-
- Strøm T, Martinussen T, Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet. 2010;375:475–80. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
