

Microbleed and microinfarct detection in amyloid angiopathy: a high-resolution MRI-histopathology study
- PMID: 27645801
- PMCID: PMC5840880
- DOI: 10.1093/brain/aww229
Microbleed and microinfarct detection in amyloid angiopathy: a high-resolution MRI-histopathology study
Abstract
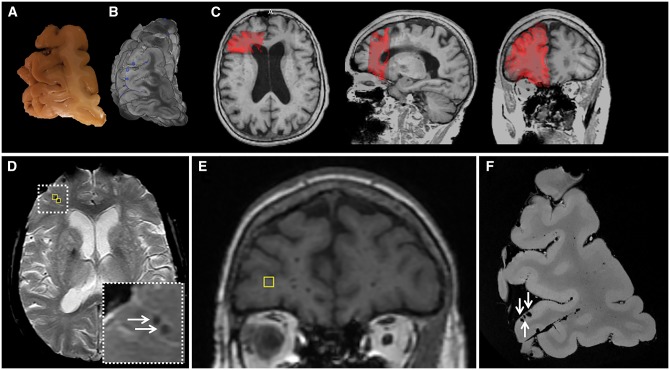
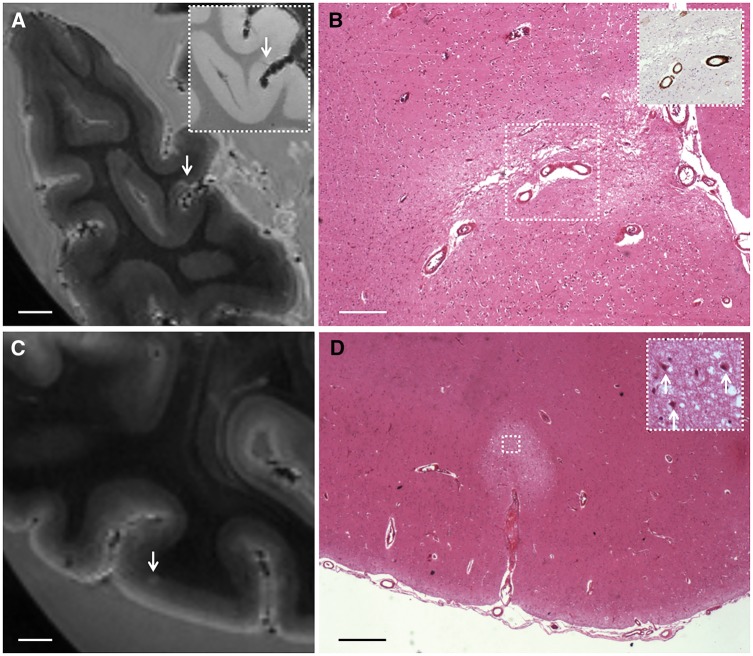
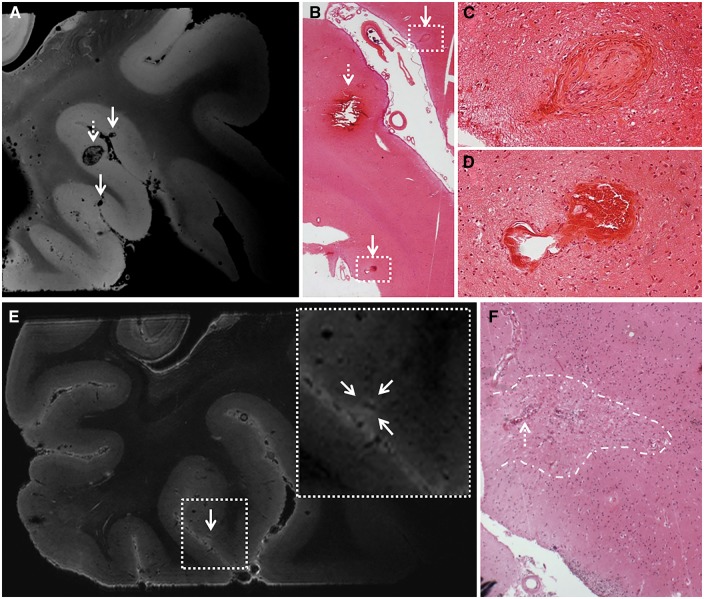
Cerebral amyloid angiopathy is a common neuropathological finding in the ageing human brain, associated with cognitive impairment. Neuroimaging markers of severe cerebral amyloid angiopathy are cortical microbleeds and microinfarcts. These parenchymal brain lesions are considered key contributors to cognitive impairment. Therefore, they are important targets for therapeutic strategies and may serve as surrogate neuroimaging markers in clinical trials. We aimed to gain more insight into the pathological basis of magnetic resonance imaging-defined microbleeds and microinfarcts in cerebral amyloid angiopathy, and to explore the pathological burden that remains undetected, by using high and ultra-high resolution ex vivo magnetic resonance imaging, as well as detailed histological sampling. Brain samples from five cases (mean age 85 ± 6 years) with pathology-proven cerebral amyloid angiopathy and multiple microbleeds on in vivo clinical magnetic resonance imaging were subjected to high-resolution ex vivo 7 T magnetic resonance imaging. On the obtained high-resolution (200 μm isotropic voxels) ex vivo magnetic resonance images, 171 microbleeds were detected compared to 66 microbleeds on the corresponding in vivo magnetic resonance images. Of 13 sampled microbleeds that were matched on histology, five proved to be acute and eight old microhaemorrhages. The iron-positive old microhaemorrhages appeared approximately four times larger on magnetic resonance imaging compared to their size on histology. In addition, 48 microinfarcts were observed on ex vivo magnetic resonance imaging in three out of five cases (two cases exhibited no microinfarcts). None of them were visible on in vivo 1.5 T magnetic resonance imaging after a retrospective analysis. Of nine sampled microinfarcts that were matched on histology, five were confirmed as acute and four as old microinfarcts. Finally, we explored the proportion of microhaemorrhage and microinfarct burden that is beyond the detection limits of ex vivo magnetic resonance imaging, by scanning a smaller sample at ultra-high resolution, followed by serial sectioning. At ultra-high resolution (75 μm isotropic voxels) magnetic resonance imaging we observed an additional 48 microbleeds (compared to high resolution), which proved to correspond to vasculopathic changes (i.e. morphological changes to the small vessels) instead of frank haemorrhages on histology. After assessing the serial sections of this particular sample, no additional haemorrhages were observed that were missed on magnetic resonance imaging. In contrast, nine microinfarcts were found in these sections, of which six were only retrospectively visible at ultra-high resolution. In conclusion, these findings suggest that microbleeds on in vivo magnetic resonance imaging are specific for microhaemorrhages in cerebral amyloid angiopathy, and that increasing the resolution of magnetic resonance images results in the detection of more 'non-haemorrhagic' pathology. In contrast, the vast majority of microinfarcts currently remain under the detection limits of clinical in vivo magnetic resonance imaging.
Keywords: histology; microbleeds; microinfarcts; post-mortem MRI; small vessel disease.
© The Author (2016). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures


References
-
- Brundel M, Heringa SM, de Bresser J, Koek HL, Zwanenburg JJ, Kappelle JL, et al. High prevalence of cerebral microbleeds at 7Tesla MRI in patients with early Alzheimer’s disease. J Alzheimers Dis 2012; 31: 259–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
