

Percutaneous Coronary Intervention Versus Optimal Medical Therapy for Stable Angina in Advanced CKD: A Decision Analysis
- PMID: 27646423
- PMCID: PMC5329119
- DOI: 10.1053/j.ajkd.2016.07.024
Percutaneous Coronary Intervention Versus Optimal Medical Therapy for Stable Angina in Advanced CKD: A Decision Analysis
Abstract
Background: Percutaneous coronary intervention (PCI) use is low in the setting of stable symptomatic angina in individuals with advanced chronic kidney disease (CKD) despite high cardiovascular risk in this population, and PCI is frequently deferred out of concern for precipitating dialysis therapy. Whether this is appropriate is uncertain, and patient-centered data comparing the relative risks and benefits of continued medical therapy versus PCI in patients with advanced CKD and stable angina are scarce.
Study design: Decision analysis.
Setting & population: Hypothetical cohort of individuals with advanced CKD (stages 4-5 with estimated glomerular filtration rates ≤ 20mL/min/1.73m2) and stable angina.
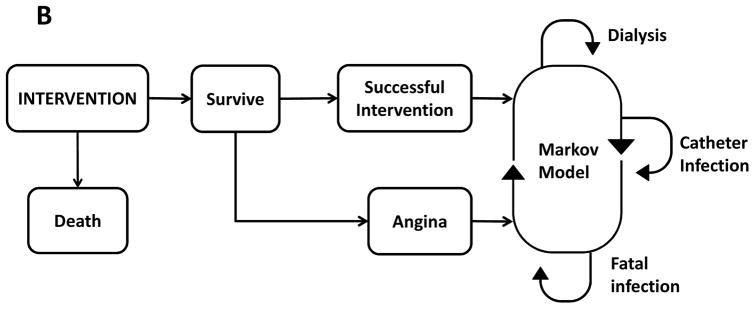
Model, perspective, & timeline: A Markov model with a Monte Carlo simulation through 12 cycles, that is, 3 years of 3-month intervals, with 10,000 microsimulations predicted mean quality-adjusted life-years.
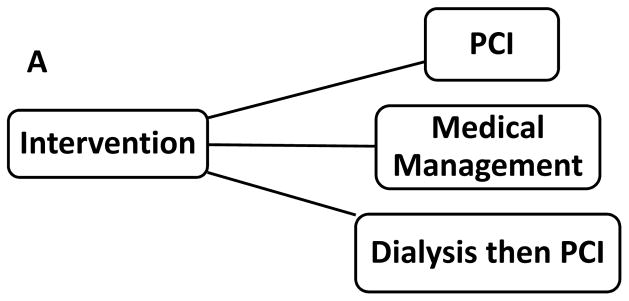
Intervention: PCI first, medical management, or dialysis (hemodialysis [HD]) followed by PCI.
Outcomes: Outcomes modeled were progression to HD therapy (for those not assigned to the preemptive HD strategy), catheter infection, and death.
Results: Our analysis showed mean quality-adjusted life-years of 1.103 ± 0.69 for PCI first, 1.088±0.70 for medical management, and 0.670±0.58 for HD followed by PCI. Probabilistic sensitivity analysis found PCI as the preferred strategy > 60% of the time.
Limitations: Values for probabilities and utilities were estimated and/or derived from multiple sources that were not uniform in their populations in terms of age, comorbid condition burden, and degree of kidney failure, and several simplifying assumptions were made.
Conclusions: Our analysis demonstrates that quality-adjusted life expectancy is similar for the PCI first and medical management strategies in patients with advanced CKD with stable angina and that the decision depends on patient preferences other than those incorporated in our model. Both strategies are superior to preemptive dialysis.
Keywords: Percutaneous coronary intervention (PCI); advanced renal failure; cardiovascular intervention; catheter infection; chronic kidney disease (CKD); contrast nephropathy; contrast-induced nephropathy (CIN); death; decision model; hemodialysis; medical management; mortality; quality of life; quality-adjusted life-year (QALY); stable angina; therapeutic nihilism.
Copyright © 2016 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Stable Angina in Advanced CKD.Am J Kidney Dis. 2017 Mar;69(3):328-330. doi: 10.1053/j.ajkd.2016.11.010. Am J Kidney Dis. 2017. PMID: 28236879 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
