

Extracorporeal life support during cardiac arrest and cardiogenic shock: a systematic review and meta-analysis
- PMID: 27647331
- PMCID: PMC5106498
- DOI: 10.1007/s00134-016-4536-8
Extracorporeal life support during cardiac arrest and cardiogenic shock: a systematic review and meta-analysis
Abstract
Purpose: Veno-arterial extracorporeal life support (ECLS) is increasingly used in patients during cardiac arrest and cardiogenic shock, to support both cardiac and pulmonary function. We performed a systematic review and meta-analysis of cohort studies comparing mortality in patients treated with and without ECLS support in the setting of refractory cardiac arrest and cardiogenic shock complicating acute myocardial infarction.
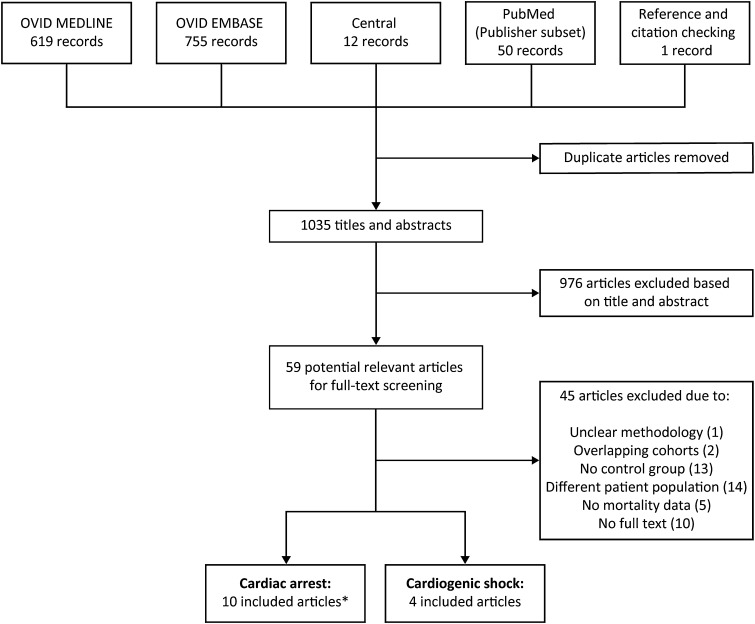
Methods: We systematically searched MEDLINE, EMBASE, the Cochrane Central Register of Controlled Trials and the publisher subset of PubMed updated to December 2015. Thirteen studies were included of which nine included cardiac arrest patients (n = 3098) and four included patients with cardiogenic shock after acute myocardial infarction (n = 235). Data were pooled by a Mantel-Haenzel random effects model and heterogeneity was examined by the I 2 statistic.
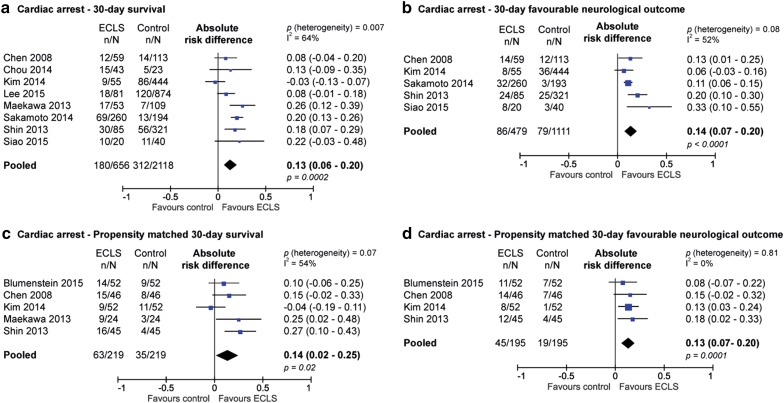
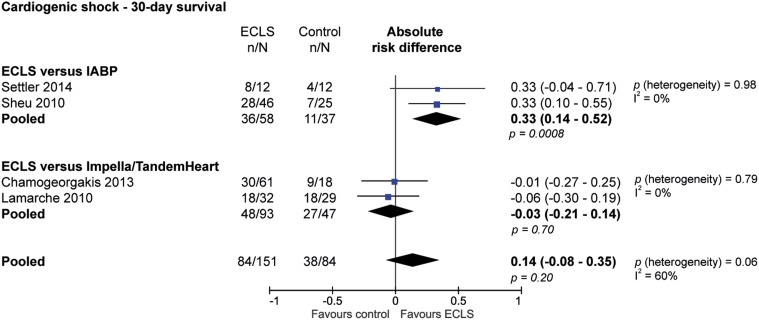
Results: In cardiac arrest, the use of ECLS was associated with an absolute increase of 30 days survival of 13 % compared with patients in which ECLS was not used [95 % CI 6-20 %; p < 0.001; number needed to treat (NNT) 7.7] and a higher rate of favourable neurological outcome at 30 days (absolute risk difference 14 %; 95 % CI 7-20 %; p < 0.0001; NNT 7.1). Propensity matched analysis, including 5 studies and 438 patients (219 in both groups), showed similar results. In cardiogenic shock, ECLS showed a 33 % higher 30-day survival compared with IABP (95 % CI, 14-52 %; p < 0.001; NNT 13) but no difference when compared with TandemHeart/Impella (-3 %; 95 % CI -21 to 14 %; p = 0.70; NNH 33).
Conclusions: In cardiac arrest, the use of ECLS was associated with an increased survival rate as well as an increase in favourable neurological outcome. In the setting of cardiogenic shock there was an increased survival with ECLS compared with IABP.
Keywords: Acute myocardial infarction; Cardiac arrest; Cardiogenic shock; Cardiopulmonary resuscitation; Extracorporeal life support; Extracorporeal membrane oxygenation; Systematic review.
Conflict of interest statement
Compliance with ethical standards Conflicts of interest J.P.S. Henriques reports research grants outside the submitted work. The other authors do not declare any conflicts of interest.
Figures
Comment in
-
Venoarterial extracorporeal membrane oxygenation for cardiac arrest/cardiogenic shock.Intensive Care Med. 2017 Jan;43(1):116-118. doi: 10.1007/s00134-016-4624-9. Epub 2016 Nov 15. Intensive Care Med. 2017. PMID: 27847983 No abstract available.
-
Extracorporeal life support during cardiac arrest and cardiogenic shock-how good is the evidence really?Ann Transl Med. 2017 Feb;5(3):58. doi: 10.21037/atm.2017.01.30. Ann Transl Med. 2017. PMID: 28251137 Free PMC article. No abstract available.
-
Meta-analysis on extracorporeal life support during cardiac arrest: do not compare apples and oranges.Ann Transl Med. 2017 Mar;5(5):119. doi: 10.21037/atm.2017.01.24. Ann Transl Med. 2017. PMID: 28361084 Free PMC article. No abstract available.
References
-
- Goldberg RJ, Spencer FA, Gore JM, Lessard D, Yarzebski J. Thirty-year trends (1975–2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation. 2009;119:1211–1219. doi: 10.1161/CIRCULATIONAHA.108.814947. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
