

Recent hip fracture trends in Sweden and Denmark with age-period-cohort effects
- PMID: 27647528
- PMCID: PMC5206266
- DOI: 10.1007/s00198-016-3768-3
Recent hip fracture trends in Sweden and Denmark with age-period-cohort effects
Abstract
This study used nationwide hip fracture data from Denmark and Sweden during 1987-2010 to examine effects of (birth) cohort and period. We found that time trends, cohort, and period effects were different in the two countries. Results also indicated that hip fracture rates may increase in the not so far future.
Introduction: The reasons for the downturn in hip fracture rates remain largely unclear but circumstances earlier in life seem important.
Methods: We ascertained hip fractures in the populations ≥50 years in Denmark and Sweden in national discharge registers. Country- and sex-specific age-period-cohort (APC) effects during 1987-2010 were evaluated by log-likelihood estimates in Poisson regression models presented as incidence rate ratios (IRR).
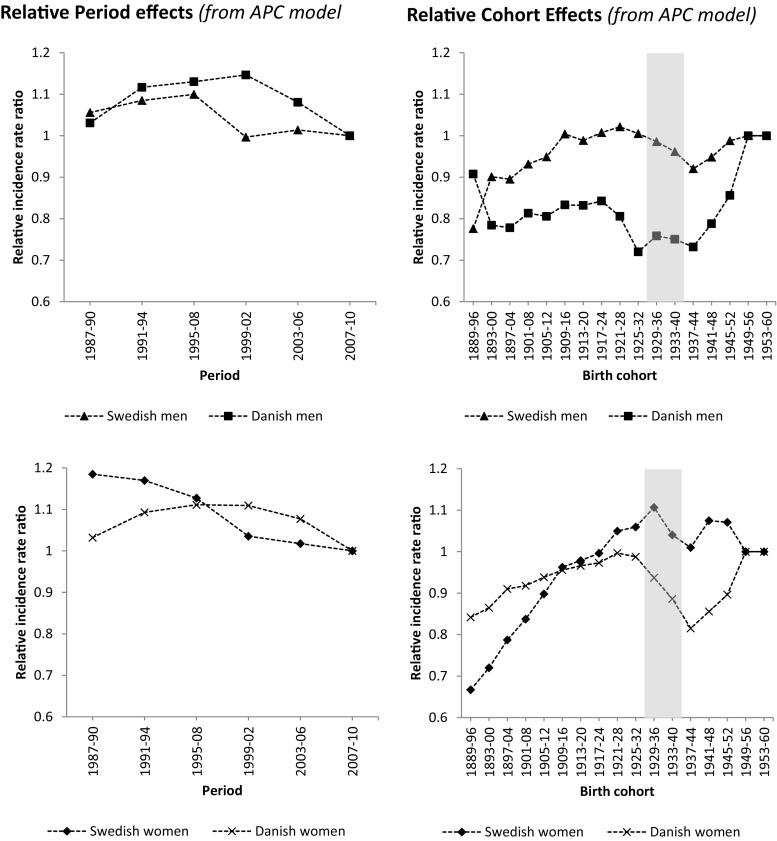
Results: There were 399,596 hip fractures in SE and 248,773 in DK. Age-standardized hip fracture rate was stable in SE men but decreased in SE women and in DK. Combined period + cohort effects were generally stronger in SE than DK and in women than men. IRR per period ranged from 1.05 to 1.30 in SE and 0.95 to 1.21 in DK. IRR per birth cohort ranged from 1.07 to 3.13 in SE and 0.77 to 1.67 in DK. Relative period effects decreased with successive period in SE and described a convex curve in DK. Relative cohort effects increased with successive birth cohort in both countries but with lower risks for DK women and men and SE women born around the 1930s (age 75-86 years today and responsible for most hip fractures) partly explaining the recent downturn. Men and women born thereafter however seem to have a higher hip fracture risk, and we expect a reversal of the present decline in rates, with increasing hip fracture rates in both Denmark and Sweden during the upcoming decade.
Conclusions: Time trends, cohort, and period effects were different in SE and DK. This may reflect differences in general health as evident in known differences in life expectancy, healthcare organization, and prevention such as use of anti-osteoporosis drugs. Analyses indicate that hip fracture rates may increase in the not so far future.
Keywords: Age-period-cohort; Hip fracture; Men; Trends; Women.
Conflict of interest statement
Compliance with ethical standards The study, which utilized only anonymized official registry data, was approved by Statistics Denmark (project reference 703857) and the ethics committee at Lund University, Sweden (2012/394). Conflicts of interest BR, JB, and CC have no potential conflicts of interest. BA has received research grants from or served as an investigator in studies for Novartis, Nycomed/Takeda, NPS Pharmaceuticals, and Amgen and has in the past served as a national advisory board member for Nycomed/Takeda, Merck, and Amgen, and received speakers fees from Nycomed/Takeda, Amgen, Merck, and Eli Lilly.
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
