

Prevalence of lactic acidaemia in patients with advanced heart failure and depressed cardiac output
- PMID: 27647751
- PMCID: PMC5359085
- DOI: 10.1002/ejhf.628
Prevalence of lactic acidaemia in patients with advanced heart failure and depressed cardiac output
Abstract
Aims: Heart failure (HF) has been defined classically as a condition in which the heart is unable to deliver sufficient oxygen to match the needs of the metabolizing tissues. Surprisingly, this definition has never been validated. The goal of this study was to determine the prevalence of elevated lactate levels in a cohort of patients with advanced heart failure.
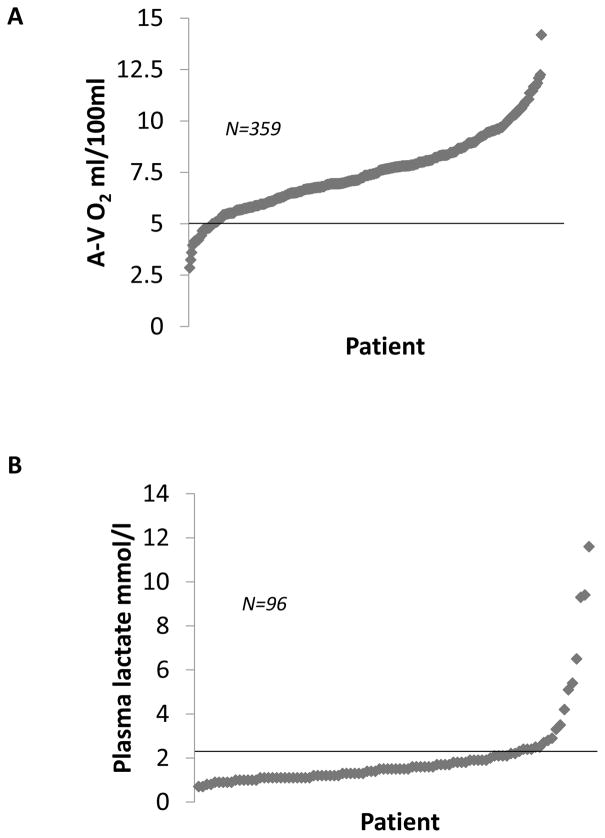
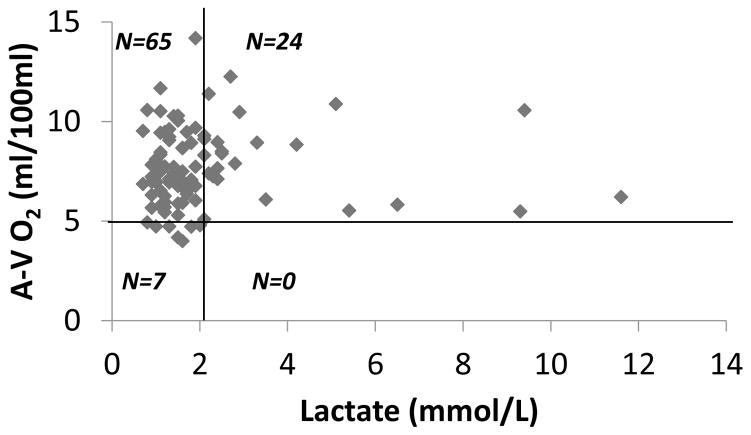
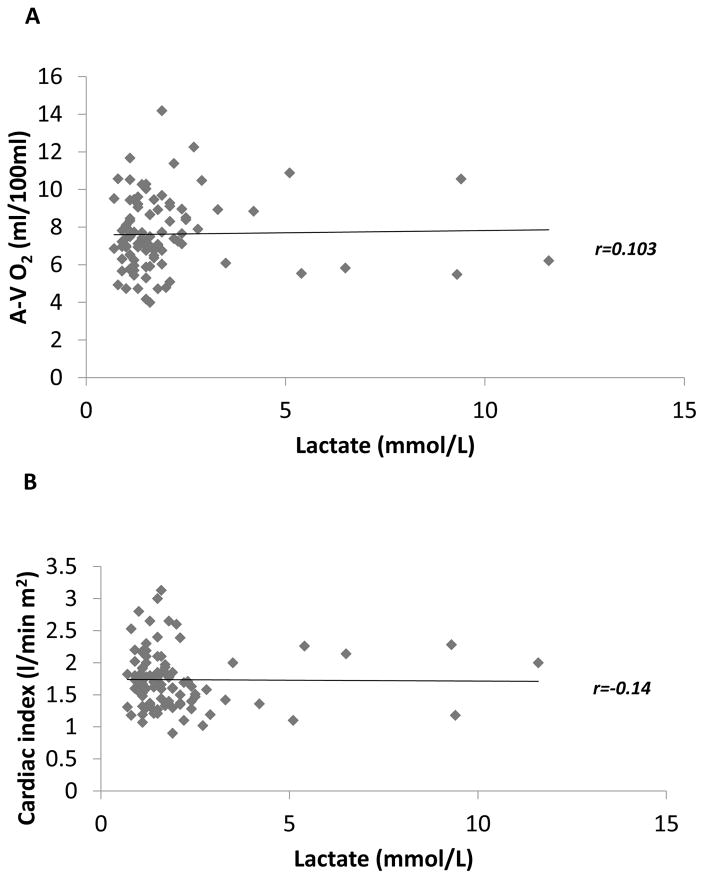
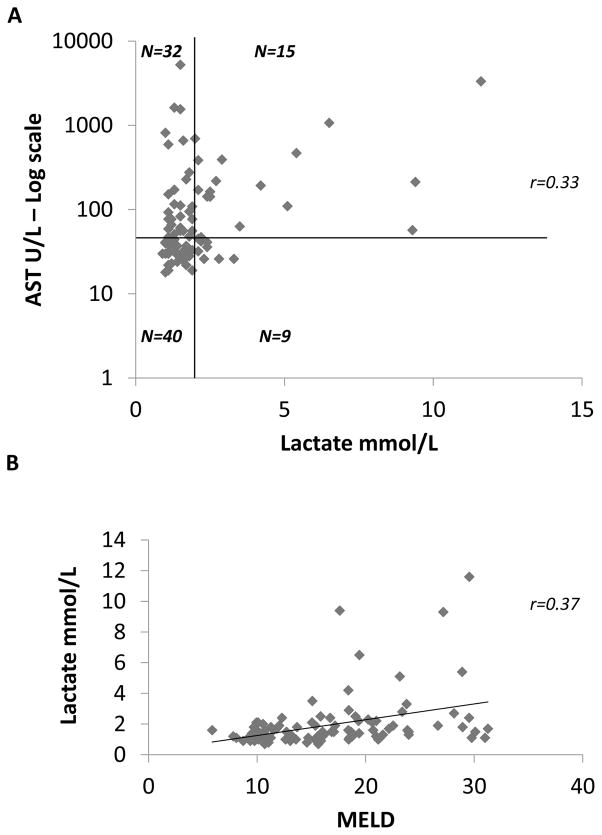
Methods and results: We retrospectively analysed the arterio-venous oxygen difference (A-V O2 ), haemodynamics, and plasma lactate levels in stage D heart failure patients who were being evaluated for a left ventricular assist device (LVAD). We identified 359 patients with a right heart catheterization (RHC) performed prior to LVAD implantation. Plasma lactate was available for 96 patients. RHC showed that 93% of the patients had an A-V O2 above the upper limit of normal (>5 mL/100 mL). Among patients with measured lactate levels, the prevalence of elevated lactate (>2.1 mmol/L) was 25% (95% confidence interval 16.7-34.9). The A-V O2 was widened in all patients with elevated lactate, but plasma lactate did not correlate with A-V O2 (r = 0.02) and only 27% of patients with increased A-V O2 had elevated plasma lactate.
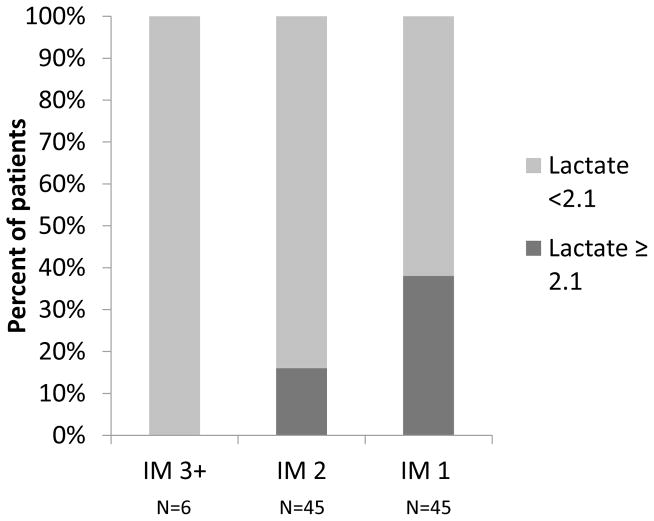
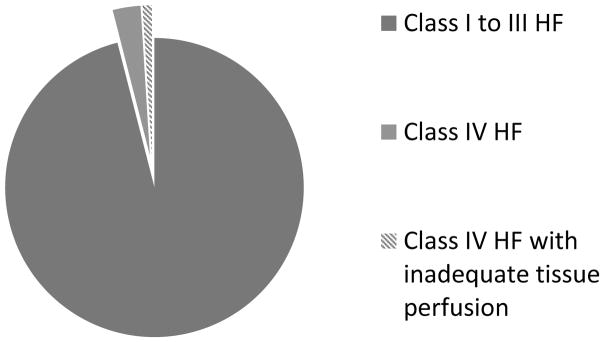
Conclusions: Lactate levels were normal in ∼75% of the patients with advanced heart failure and a widened A-V O2 , suggesting that the cardiac output was sufficient to meet the metabolic needs of the peripheral metabolizing tissues. Given that ∼4% of heart failure patients are in NYHA class IV, these findings suggest that the classic definition of heart failure pertains to ∼1% of patients with HF.
Keywords: Cardiac output; Heart failure with reduced ejection fraction; Lactic acid; Left ventricular assist device.
© 2016 The Authors. European Journal of Heart Failure © 2016 European Society of Cardiology.
Conflict of interest statement
Figures
Comment in
-
Does a normal peripheral lactate value always indicate an aerobic tissue metabolism?Eur J Heart Fail. 2017 Aug;19(8):1034-1035. doi: 10.1002/ejhf.863. Epub 2017 May 25. Eur J Heart Fail. 2017. PMID: 28547836 No abstract available.
References
-
- Mann DL. The evolution of modern theory and therapy for heart faillure. Prog Ped Cardiol. 2014;37:9–12.
-
- Braunwald E. Heart failure. JACC Heart Fail. 2013;1:1–20. - PubMed
-
- Francis GS, Wilson Tang WH, Walsh RA. Pathophysiology of Heart Failure. In: Fuster V, Walsh RA, Harrington RA, editors. Hurst’s The Heart. 13. McGraw-Hill Companies; 2011.
-
- Henes J, Rosenberger P. Systolic heart failure: diagnosis and therapy. Curr Opin Anaesthesiol. 2016;29:55–60. - PubMed
-
- Hobbs B. Heart Failure. In: Carey WD, editor. Cleveland Clinic current Clinical Medicine. 2. Saunders Elsevier; 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
