

Predicting the Individual Risk of Acute Severe Colitis at Diagnosis
- PMID: 27647858
- PMCID: PMC5881607
- DOI: 10.1093/ecco-jcc/jjw159
Predicting the Individual Risk of Acute Severe Colitis at Diagnosis
Abstract
Background and aims: Acute severe colitis [ASC] is associated with major morbidity. We aimed to develop and externally validate an index that predicted ASC within 3 years of diagnosis.
Methods: The development cohort included patients aged 16-89 years, diagnosed with ulcerative colitis [UC] in Oxford and followed for 3 years. Primary outcome was hospitalization for ASC, excluding patients admitted within 1 month of diagnosis. Multivariable logistic regression examined the adjusted association of seven risk factors with ASC. Backwards elimination produced a parsimonious model that was simplified to create an easy-to-use index. External validation occurred in separate cohorts from Cambridge, UK, and Uppsala, Sweden.
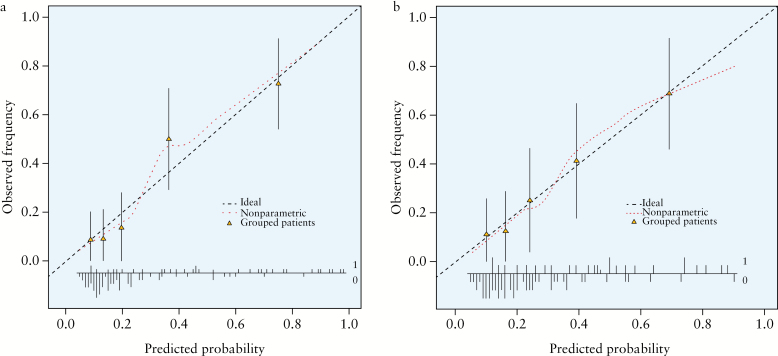
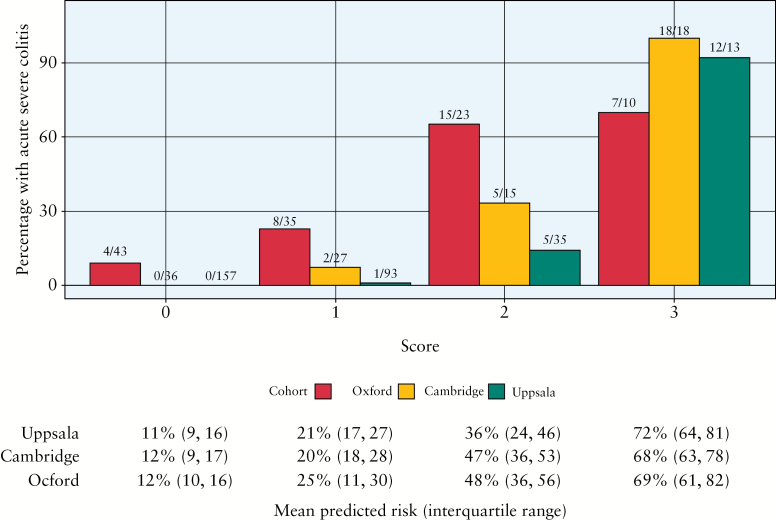
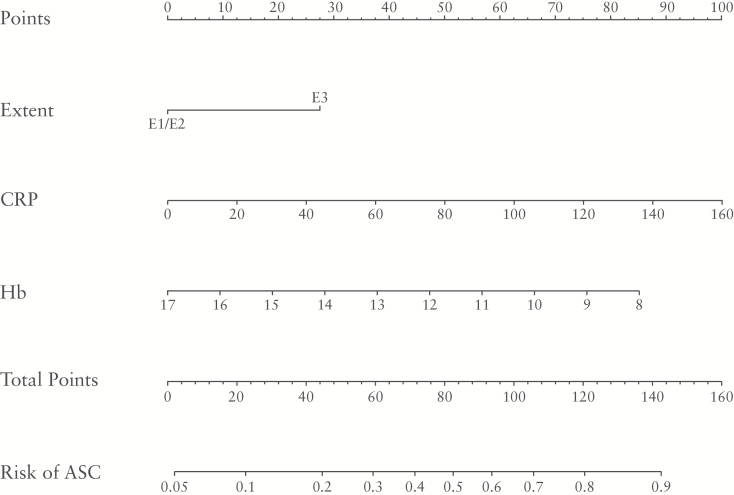
Results: The development cohort [Oxford] included 34/111 patients who developed ASC within a median 14 months [range 1-29]. The final model applied the sum of 1 point each for extensive disease, C-reactive protein [CRP] > 10mg/l, or haemoglobin < 12g/dl F or < 14g/dl M at diagnosis, to give a score from 0/3 to 3/3. This predicted a 70% risk of developing ASC within 3 years [score 3/3]. Validation cohorts included different proportions with ASC [Cambridge = 25/96; Uppsala = 18/298]. Of those scoring 3/3 at diagnosis, 18/18 [Cambridge] and 12/13 [Uppsala] subsequently developed ASC. Discriminant ability [c-index, where 1.0 = perfect discrimination] was 0.81 [Oxford], 0.95 [Cambridge], 0.97 [Uppsala]. Internal validation using bootstrapping showed good calibration, with similar predicted risk across all cohorts. A nomogram predicted individual risk.
Conclusions: An index applied at diagnosis reliably predicts the risk of ASC within 3 years in different populations. Patients with a score 3/3 at diagnosis may merit early immunomodulator therapy.
Keywords: Biomarkers; acute severe colitis; clinical trials; prediction; ulcerative colitis.
Copyright © 2016 European Crohn’s and Colitis Organisation (ECCO). Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com
Figures
References
-
- Dignass A, Eliakim R, Magro F, et al. ; for the European Crohn’s and Colitis Organization [ECCO]. The second European consensus on the diagnosis and management of ulcerative colitis: definitions and diagnosis. J Crohns Colitis 2012;6:965–90. - PubMed
-
- Dinesen LC, Walsh AJ, Protic MN, et al. The pattern and outcome of acute severe colitis. J Crohns Colitis 2010;4: 431–7. - PubMed
-
- Lynch RW, Lowe D, Protheroe A, et al. Outcomes of rescue therapy in acute severe ulcerative colitis: data from the United Kingdom inflammatory bowel disease audit. Aliment Pharmacol Ther 2013;38:935–45. - PubMed
-
- Loly C, Belaiche J, Louis E. Predictors of severe Crohn’s disease. Scand J Gastroenterol 2008;43:948–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
