

Radiotherapy with or without temozolomide in elderly patients aged ≥ 70 years with glioblastoma
- PMID: 27647990
- PMCID: PMC5013689
- DOI: 10.5114/wo.2016.61569
Radiotherapy with or without temozolomide in elderly patients aged ≥ 70 years with glioblastoma
Abstract
Introduction: Although the recommended optimal treatment of glioblastoma multiforme (GBM) is adjuvant chemoradiotherapy, trials in GBM have excluded patients older than 70 years. In this study, we aimed to assess overall survival (OS) and prognostic factors in elderly patients (≥ 70 years) with newly diagnosed GBM treated with radiotherapy (RT) ± concurrent/adjuvant temozolomide (TMZ).
Material and methods: Inclusion criteria were patients ≥ 70 years, pre-RT Karnofsky performance status (KPS) ≥ 60, and time between diagnosis and start of RT ≤ 2 months. A total of 40 patients aged ≥ 70 years, 12 female and 28 male, treated between January 2004 and December 2012, were evaluated. Median age was 73.5 years (range, 70-83 years). The median RT dose was 60 Gy (range, 30-62 Gy). Twenty-one (52.5%) received concurrent TMZ, and of those 12 (30%) went on to receive adjuvant TMZ.
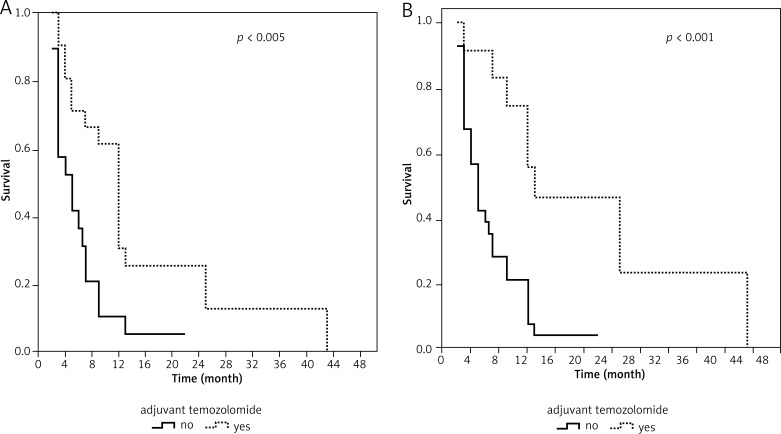
Results: The median OS was 7 months (95% CI: 5.45-8.54). One- and two-year OS for the whole cohort was 38% and 16%, respectively. Sex, type of surgery, tumor size, and RT dose did not significantly affect the OS. Presence of concurrent TMZ (p < 0.005) and presence of adjuvant TMZ (p < 0.001) were associated with longer OS in our cohort.
Conclusions: RT ± TMZ seems to be a well-tolerated treatment in patients ≥ 70 years with GBM. Even though no superiority was found between conventional or hypofractionated RT regimens (p = 0.405), the addition of concurrent and adjuvant TMZ to RT increased the OS in our study.
Keywords: elderly; glioblastoma; prognostic factors; radiotherapy; temozolomide.
Figures
References
-
- Stark AM, Stepper W, Mehdorn HM. Outcome evaluation in glioblastoma patients using different ranking scores: KPS, GOS, mRS and MRC. Eur J Cancer Care (Engl) 2010;19:39–44. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96. - PubMed
-
- Oh SW, Jee TK, Kong DS, Nam DH, Lee JI, Seol HJ. Outcome of conventional treatment and prognostic factor in elderly glioblastoma patients. Acta Neurochir (Wien) 2014;156:641–51. - PubMed
-
- Niyazi M, Schwarz SB, Suchorska B, Belka C. Radiotherapy with and without temozolomide in elderly patients with glioblastoma. Strahlenther Onkol. 2012;188:154–9. - PubMed
-
- Fiorentino A, De Bonis P, Chiesa S, Balducci M, Fusco V. Elderly patients with glioblastoma: the treatment challenge. Expert Rev Neurother. 2013;13:1099–105. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources