

Clinical implementation of a novel applicator in high-dose-rate brachytherapy treatment of esophageal cancer
- PMID: 27648086
- PMCID: PMC5018528
- DOI: 10.5114/jcb.2016.61933
Clinical implementation of a novel applicator in high-dose-rate brachytherapy treatment of esophageal cancer
Abstract
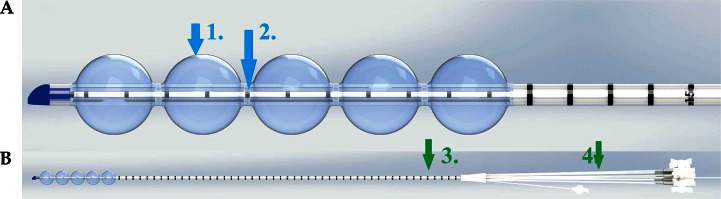
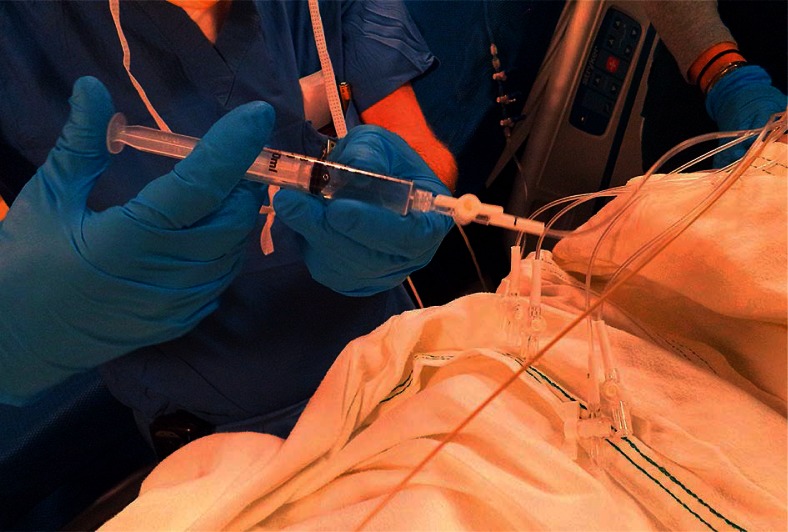
Purpose: In this study, we present the clinical implementation of a novel transoral balloon centering esophageal applicator (BCEA) and the initial clinical experience in high-dose-rate (HDR) brachytherapy treatment of esophageal cancer, using this applicator.
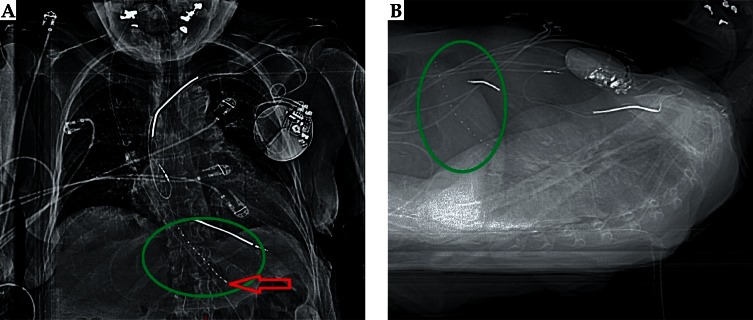
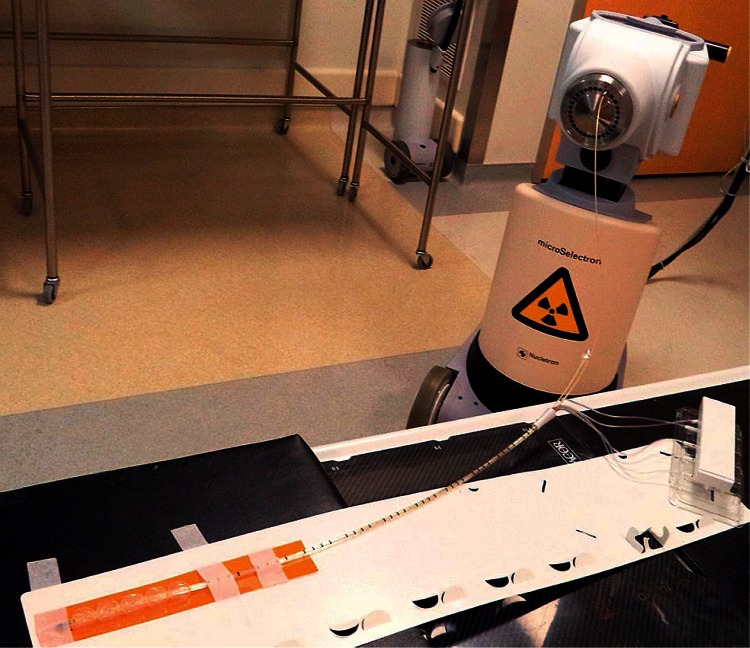
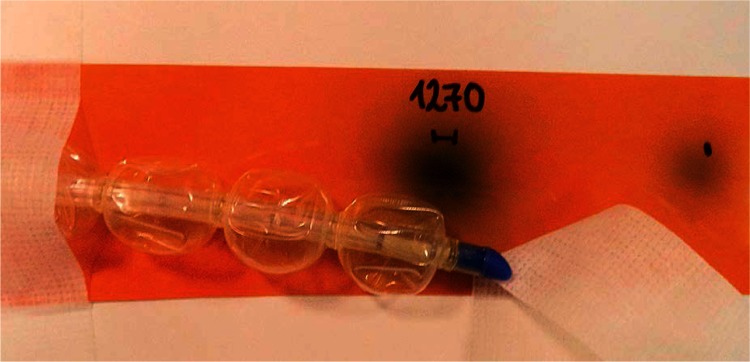
Material and methods: Acceptance testing and commissioning of the BCEA were performed prior to clinical use. Full performance testing was conducted including measurements of the dimensions and the catheter diameter, evaluation of the inflatable balloon consistency, visibility of the radio-opaque markers, congruence of the markers, absolute and relative accuracy of the HDR source in the applicator using the radiochromic film and source position simulator, visibility and digitization of the applicator on the computed tomography (CT) images under the clinical conditions, and reproducibility of the offset. Clinical placement of the applicator, treatment planning, treatment delivery, and patient's response to the treatment were elaborated as well.
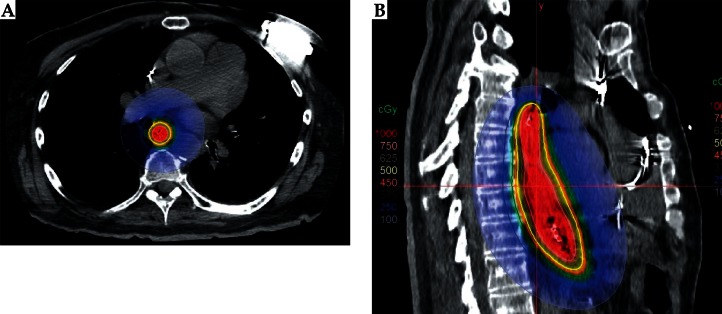
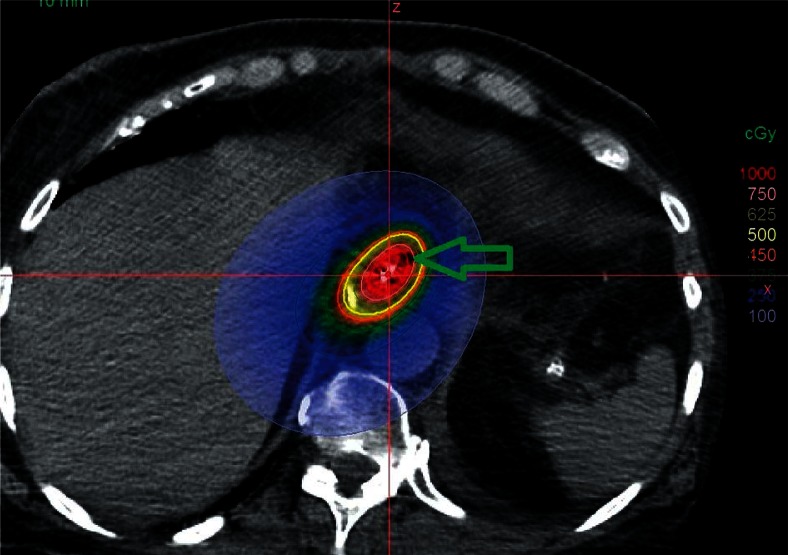
Results: The experiments showed sub-millimeter accuracy in the source positioning with distal position at 1270 mm. The digitization (catheter reconstruction) was uncomplicated due to the good visibility of markers. The treatment planning resulted in a favorable dose distribution. This finding was pronounced for the treatment of the curvy anatomy of the lesion due to the improved repeatability and consistency of the delivered fractional dose to the patient, since the radioactive source was placed centrally within the lumen with respect to the clinical target due to the five inflatable balloons.
Conclusions: The consistency of the BCEA positioning resulted in the possibility to deliver optimized non-uniform dose along the catheter, which resulted in an increase of the dose to the cancerous tissue and lower doses to healthy tissue. A larger number of patients and long-term follow-up will be required to investigate if the delivered optimized treatment can lead to improved clinical outcomes.
Keywords: HDR; brachytherapy; esophageal cancer; optimization.
Figures
References
-
- Gaspar LE, Nag S, Herskovic A, et al. Clinical Research Committee. American Brachytherapy Society (ABS) consensus guidelines for brachytherapy of esophageal cancer. Int J Radiat Oncol Biol Phys. 1997;38:127–132. - PubMed
-
- Gaspar LE. Radiation therapy for esophageal cancer: improving the therapeutic ratio. Semin Radiat Oncol. 1994;4:192–201. - PubMed
-
- Sharma V, Mahantshetty U, Dinshaw KA, et al. Palliation of advanced/recurrent esophageal carcinoma with high-dose-rate brachytherapy. Int J Radiat Oncol Biol Phys. 2002;52:310–315. - PubMed
-
- Mahantshetty U, Dinshaw K, Sharma V. Palliation of advanced/recurrent carcinoma esophagus with intraluminal brachytherapy. Ind J Thor Cardiovascr Surg. 2003;19:119–123.
-
- Skowronek J, Adamska K, Suwalska M, et al. Palliative HDR brachytherapy in treatment of advanced esophageal cancer. Rep Pract Oncol Radiother. 2000;5:111–119.
LinkOut - more resources
Full Text Sources
Other Literature Sources