

Chronic Kidney Disease in Primary Care: Outcomes after Five Years in a Prospective Cohort Study
- PMID: 27648564
- PMCID: PMC5029805
- DOI: 10.1371/journal.pmed.1002128
Chronic Kidney Disease in Primary Care: Outcomes after Five Years in a Prospective Cohort Study
Abstract
Background: Chronic kidney disease (CKD) is commonly managed in primary care, but most guidelines have a secondary care perspective emphasizing the risk of end-stage kidney disease (ESKD) and need for renal replacement therapy. In this prospective cohort study, we sought to study in detail the natural history of CKD in primary care to better inform the appropriate emphasis for future guidance.
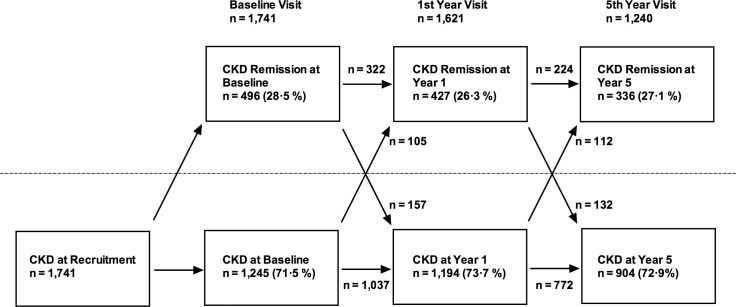
Methods and findings: In this study, 1,741 people with CKD stage 3 were individually recruited from 32 primary care practices in Derbyshire, United Kingdom. Study visits were undertaken at baseline, year 1, and year 5. Binomial logistic regression and Cox proportional hazards models were used to model progression, CKD remission, and all-cause mortality. We used Kidney Disease: Improving Global Outcomes (KDIGO) criteria to define CKD progression and defined CKD remission as the absence of diagnostic criteria (estimated glomerular filtration rate [eGFR] >60 ml/min/1.73 m2 and urine albumin-to-creatinine ratio [uACR] <3 mg/mmol) at any study visit. Participants were predominantly elderly (mean ± standard deviation (SD) age 72.9 ± 9.0 y), with relatively mild reduction in GFR (mean ± SD eGFR 53.5 ± 11.8 mL/min/1,73 m2) and a low prevalence of albuminuria (16.9%). After 5 y, 247 participants (14.2%) had died, most of cardiovascular causes. Only 4 (0.2%) developed ESKD, but 308 (17.7%) evidenced CKD progression by KDIGO criteria. Stable CKD was observed in 593 participants (34.1%), and 336 (19.3%) met the criteria for remission. Remission at baseline and year 1 was associated with a high likelihood of remission at year 5 (odds ratio [OR] = 23.6, 95% CI 16.5-33.9 relative to participants with no remission at baseline and year 1 study visits). Multivariable analyses confirmed eGFR and albuminuria as key risk factors for predicting adverse as well as positive outcomes. Limitations of this study include reliance on GFR estimated using the Modification of Diet in Renal Disease study (MDRD) equation for recruitment (but not subsequent analysis) and a study population that was predominantly elderly and white, implying that the results may not be directly applicable to younger populations of more diverse ethnicity.
Conclusions: Management of CKD in primary care should focus principally on identifying the minority of people at high risk of adverse outcomes, to allow intervention to slow CKD progression and reduce cardiovascular events. Efforts should also be made to identify and reassure the majority who are at low risk of progression to ESKD. Consideration should be given to adopting an age-calibrated definition of CKD to avoid labelling a large group of people with age-related decline in GFR and low associated risk as having CKD.
Conflict of interest statement
MWT is a member of the PLOS Medicine editorial board.
Figures

Comment in
-
Interplay between Diagnostic Criteria and Prognostic Accuracy in Chronic Kidney Disease.PLoS Med. 2016 Sep 20;13(9):e1002129. doi: 10.1371/journal.pmed.1002129. eCollection 2016 Sep. PLoS Med. 2016. PMID: 27648826 Free PMC article.
-
Chronic kidney disease: Outcomes of CKD in primary care.Nat Rev Nephrol. 2016 Dec;12(12):714. doi: 10.1038/nrneph.2016.148. Epub 2016 Oct 10. Nat Rev Nephrol. 2016. PMID: 27721377 No abstract available.
-
A rose by any other name: is stage 3a chronic kidney disease really a disease?Kidney Int. 2017 Jan;91(1):6-8. doi: 10.1016/j.kint.2016.11.005. Kidney Int. 2017. PMID: 28003092
References
-
- James MT, Grams ME, Woodward M, Elley CR, Green JA, Wheeler DC, et al. A Meta-analysis of the Association of Estimated GFR, Albuminuria, Diabetes Mellitus, and Hypertension With Acute Kidney Injury. American journal of kidney diseases: the official journal of the National Kidney Foundation. 2015;66(4):602–12. 10.1053/j.ajkd.2015.02.338 . - DOI - PMC - PubMed
-
- Matsushita K, Coresh J, Sang Y, Chalmers J, Fox C, Guallar E, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. The lancet Diabetes & endocrinology. 2015;3(7):514–25. 10.1016/S2213-8587(15)00040-6 . - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
