

Rosacea: Molecular Mechanisms and Management of a Chronic Cutaneous Inflammatory Condition
- PMID: 27649161
- PMCID: PMC5037831
- DOI: 10.3390/ijms17091562
Rosacea: Molecular Mechanisms and Management of a Chronic Cutaneous Inflammatory Condition
Abstract
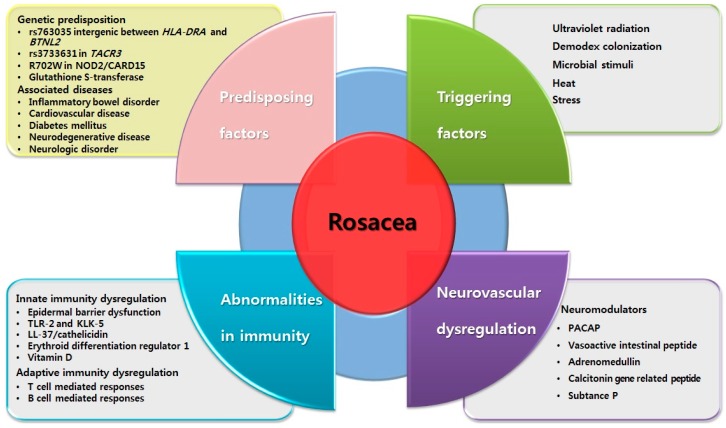
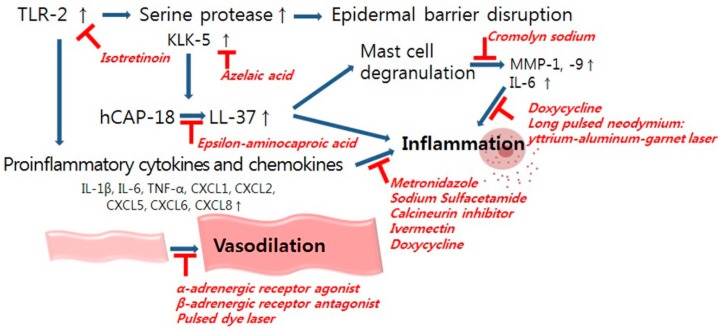
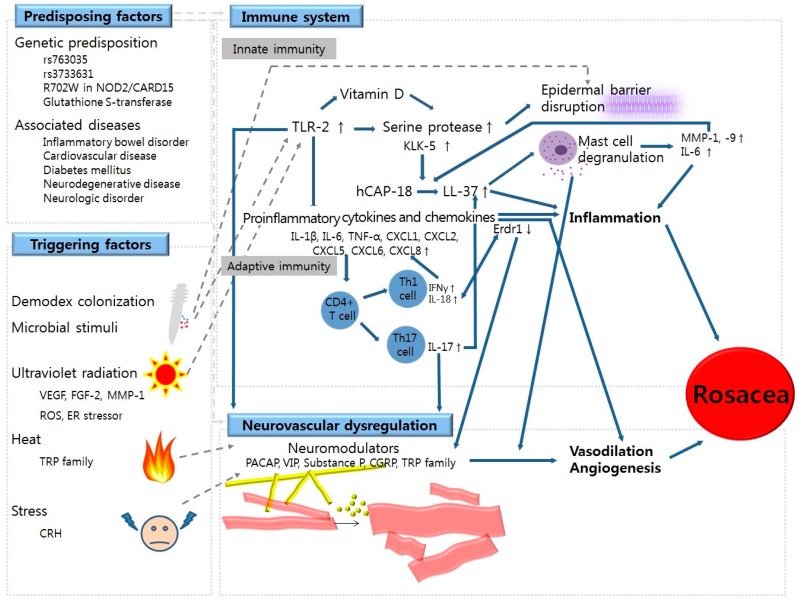
Rosacea is a chronic cutaneous inflammatory disease that affects the facial skin. Clinically, rosacea can be categorized into papulopustular, erythematotelangiectatic, ocular, and phymatous rosacea. However, the phenotypic presentations of rosacea are more heterogeneous. Although the pathophysiology of rosacea remains to be elucidated, immunologic alterations and neurovascular dysregulation are thought to have important roles in initiating and strengthening the clinical manifestations of rosacea. In this article, we present the possible molecular mechanisms of rosacea based on recent laboratory and clinical studies. We describe the genetic predisposition for rosacea along with its associated diseases, triggering factors, and suggested management options in detail based on the underlying molecular biology. Understanding the molecular pathomechanisms of rosacea will likely aid toward better comprehending its complex pathogenesis.
Keywords: genetic; immune defect; inflammation; neurovascular dysregulation; rosacea; triggering factor.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
