

The Diagnosis of Delirium Superimposed on Dementia: An Emerging Challenge
- PMID: 27650668
- PMCID: PMC5373084
- DOI: 10.1016/j.jamda.2016.07.014
The Diagnosis of Delirium Superimposed on Dementia: An Emerging Challenge
Abstract
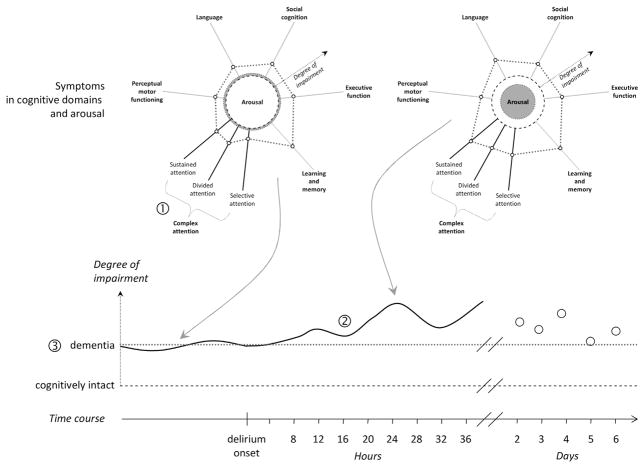
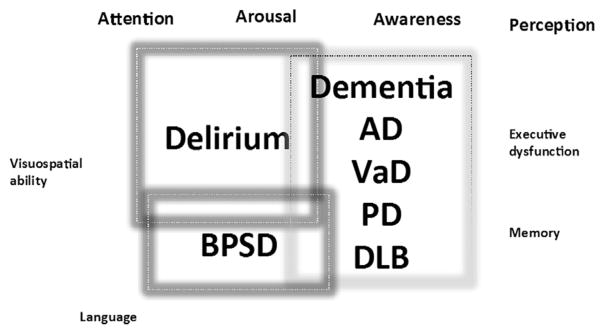
Delirium occurring in patients with dementia is referred to as delirium superimposed on dementia (DSD). People who are older with dementia and who are institutionalized are at increased risk of developing delirium when hospitalized. In addition, their prior cognitive impairment makes detecting their delirium a challenge. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision are considered the standard reference for the diagnosis of delirium and include criteria of impairments in cognitive processes such as attention, additional cognitive disturbances, or altered level of arousal. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision does not provide guidance regarding specific tests for assessment of the cognitive process impaired in delirium. Importantly, the assessment or inclusion of preexisting cognitive impairment is also not addressed by these standards. The challenge of DSD gets more complex as types of dementia, particularly dementia with Lewy bodies, which has features of both delirium and dementia, are considered. The objective of this article is to critically review key elements for the diagnosis of DSD, including the challenge of neuropsychological assessment in patients with dementia and the influence of particular tests used to diagnose DSD. To address the challenges of DSD diagnosis, we present a framework for guiding the focus of future research efforts to develop a reliable reference standard to diagnose DSD. A key feature of a reliable reference standard will improve the ability to clinically diagnose DSD in facility-based patients and research studies.
Keywords: Alzheimer disease; Delirium; Lewy Body dementia; delirium superimposed on dementia; dementia; diagnosis.
Copyright © 2016 AMDA – The Society for Post-Acute and Long-Term Care Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Fick DM, Agostini JV, Inouye SK. Delirium superimposed on dementia: A systematic review. J Am Geriatr Soc. 2002;50:1723–1732. - PubMed
-
- de Lange E, Verhaak PF, van der Meer K. Prevalence, presentation and prognosis of delirium in older people in the population, at home and in long term care: A review. Int J Geriatr psychiatry. 2013;28:127–134. - PubMed
-
- Sampson EL, Blanchard MR, Jones L, et al. Dementia in the acute hospital: Prospective cohort study of prevalence and mortality. Br J Psychiatry. 2009;195:61–66. - PubMed
-
- Bellelli G, Frisoni GB, Turco R, et al. Delirium superimposed on dementia predicts 12-month survival in elderly patients discharged from a postacute rehabilitation facility. J Gerontol Ser A Biol Sci Med Sci. 2007;62:1306–1309. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
