

Iatrogenic Hip Instability Is a Devastating Complication After the Modified Dunn Procedure for Severe Slipped Capital Femoral Epiphysis
- PMID: 27650993
- PMCID: PMC5339129
- DOI: 10.1007/s11999-016-5094-7
Iatrogenic Hip Instability Is a Devastating Complication After the Modified Dunn Procedure for Severe Slipped Capital Femoral Epiphysis
Abstract
Background: The modified Dunn procedure facilitates femoral capital realignment for slipped capital femoral epiphysis (SCFE) through a surgical hip dislocation approach. Iatrogenic postoperative hip instability after this procedure has not been studied previously; however, we were concerned when we observed several instances of this serious complication, and we wished to study it further.
Questions/purposes: The purpose of this study was to evaluate the frequency, timing, and clinical presentation (including complications) associated with iatrogenic instability after the modified Dunn procedure for SCFE.
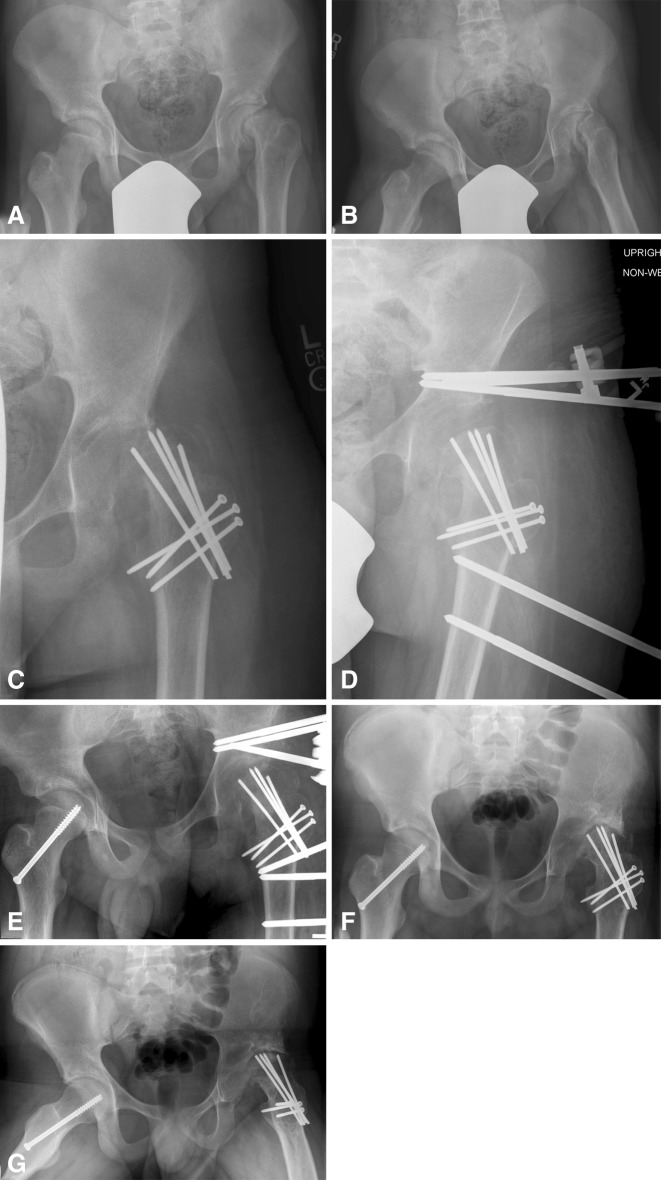
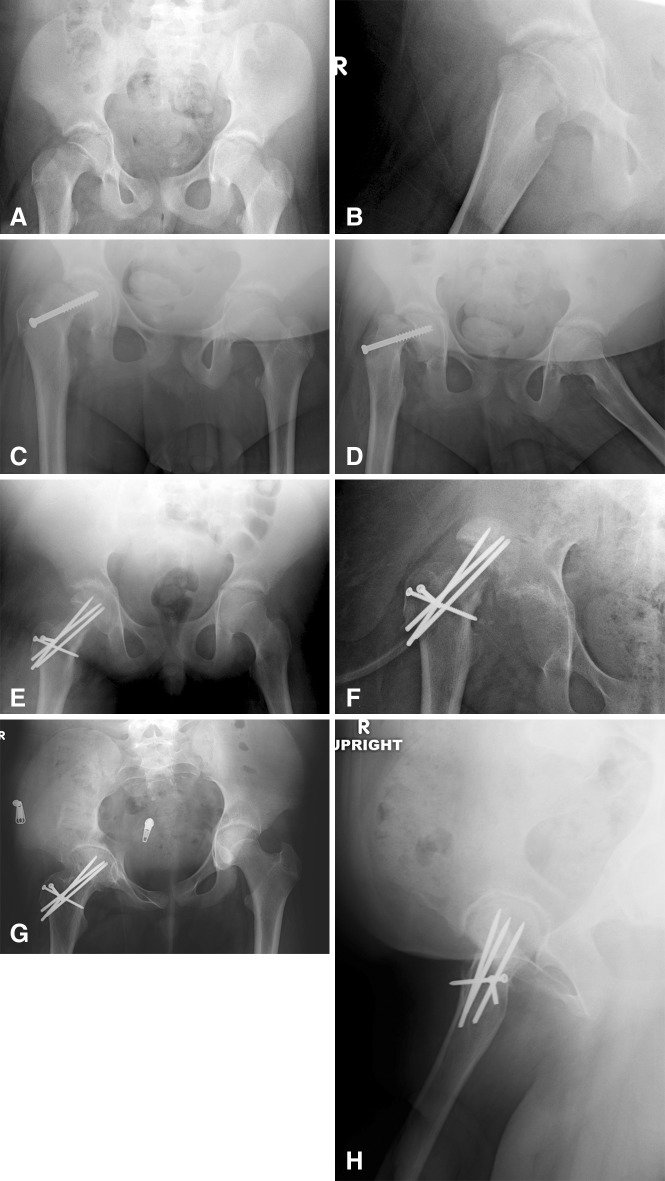
Methods: Between 2007 and 2014, eight international institutions performed the modified Dunn procedure through a surgical dislocation approach in 406 patients. During the period in question, indications varied at those sites, but the procedure was used only in a minority of their patients treated surgically for SCFE (31% [406 of 1331]) with the majority treated with in situ fixation. It generally was performed for patients with severe deformity with a slip angle greater than 40°. Institutional databases were searched for all patients with SCFE who developed postoperative hip instability defined as hip subluxation or dislocation of the involved hip during the postoperative period. We reviewed in detail the clinical notes and operative records of those who presented with instability. We obtained demographic information, time from slip to surgery, type of fixation, operative details, and clinical course including the incidence of complications. Followup on those patients with instability was at a mean of 2 years (range, 1-5 years) after the index procedure. Complications were graded according to the modified Dindo-Clavien classification. Radiographic images were reviewed to measure the preoperative slip angle and the presence of osteonecrosis.
Results: A total of 4% of patients treated with the modified Dunn procedure developed postoperative hip instability (17 of 406). Mean age of the patients was 13 years (range, 9-16 years). Instability presented as persistent hip pain in the postoperative period or was incidentally identified radiographically during the postoperative visit and occurred at a median of 3 weeks (range, 1 day to 2 months) after the modified Dunn procedure. Eight patients underwent revision surgery to address the postoperative instability. Fourteen of 17 patients developed femoral head avascular necrosis and three of 17 patients underwent THA during this short-term followup.
Conclusions: Anterolateral hip instability after the modified Dunn procedure for severe, chronic SCFE is an uncommon yet potentially devastating complication. Future studies might evaluate the effectiveness of maintaining anterior hip precautions for several weeks postoperatively in an abduction brace or broomstick cast to prevent this complication.
Level of evidence: Level IV, therapeutic study.
Figures
Comment in
-
CORR Insights®: Iatrogenic Hip Instability Is a Devastating Complication After the Modified Dunn Procedure for Severe Slipped Capital Femoral Epiphysis.Clin Orthop Relat Res. 2017 Apr;475(4):1236-1238. doi: 10.1007/s11999-016-5141-4. Epub 2016 Oct 31. Clin Orthop Relat Res. 2017. PMID: 27796803 Free PMC article. No abstract available.
References
-
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–213. doi: 10.1097/01.sla.0000133083.54934.ae. - DOI - PMC - PubMed
-
- Dunn DM. The treatment of adolescent slipping of the upper femoral epiphysis. J Bone Joint Surg Br. 1964;46:621–629. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
