

Rare case of bilateral traumatic internal carotid artery dissection
- PMID: 27651410
- PMCID: PMC5030602
- DOI: 10.1136/bcr-2016-217262
Rare case of bilateral traumatic internal carotid artery dissection
Abstract
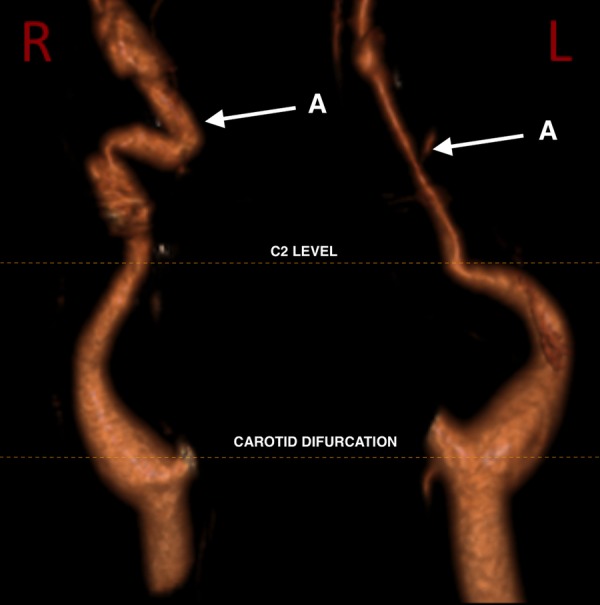
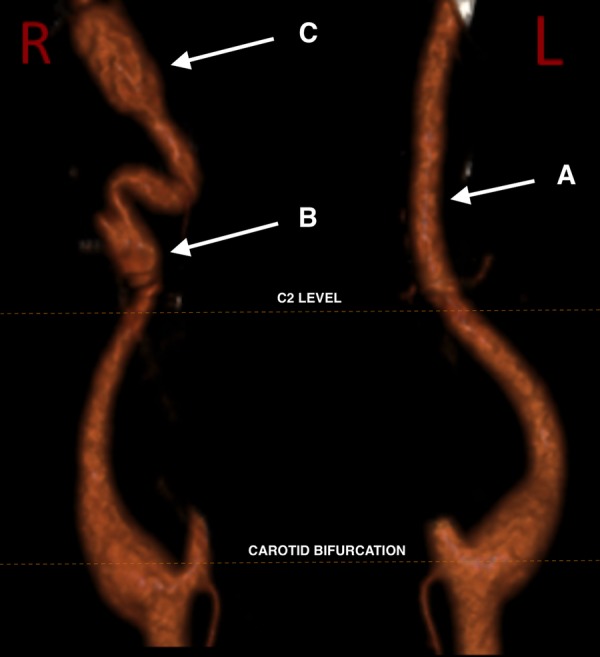
A 55-year-old man was working in a trench when the wall collapsed in on him, pinning him to the wall. On arrival in the emergency department the patient began reporting of right-sided headache. Neurological examination revealed left-sided reduced sensation with weakness. Whole-body CT scan showed right-sided flail chest and bilateral haemothorax as well as loss of flow and thinning of the distal right internal carotid artery (ICA) and loss of grey white matter differentiation in keeping with traumatic ICA dissection with a right middle cerebral artery (MCA) infarct. He was started on aspirin 300 mg once daily. 3 days postadmission the patient experienced worsening of vision and expressive dysphasia. CT angiogram showed bilateral ICA dissections extending from C2 to the skull base. The patient was managed conservatively in the stroke unit for infarction and was discharged home for follow-up in stroke clinic.
2016 BMJ Publishing Group Ltd.
Figures

Similar articles
-
Isolated oculomotor nerve palsy: a rare manifestation of internal carotid artery dissection.BMJ Case Rep. 2014 Oct 16;2014:bcr2014205413. doi: 10.1136/bcr-2014-205413. BMJ Case Rep. 2014. PMID: 25323280 Free PMC article.
-
Internal carotid artery dissection heralded by an oculomotor nerve palsy: case report and literature review.Neurologist. 2011 Nov;17(6):333-7. doi: 10.1097/NRL.0b013e318218030a. Neurologist. 2011. PMID: 22045285
-
Fibromuscular dysplasia with carotid artery dissection presenting as an isolated hemianopsia.J Stroke Cerebrovasc Dis. 2007 May-Jun;16(3):130-4. doi: 10.1016/j.jstrokecerebrovasdis.2006.12.002. J Stroke Cerebrovasc Dis. 2007. PMID: 17689408
-
[Spontaneous intracranial internal carotid artery dissection: 6 case reports and a review of 39 cases in the literature].Rinsho Shinkeigaku. 2003 Jun;43(6):313-21. Rinsho Shinkeigaku. 2003. PMID: 14503348 Review. Japanese.
-
[Spontaneous improvement of idiopathic intracranial carotid artery dissection: a case report].No Shinkei Geka. 2008 Jul;36(7):625-31. No Shinkei Geka. 2008. PMID: 18634405 Review. Japanese.
Cited by
-
Bilateral Blunt Traumatic Dissections of the Extracranial Internal Carotid Artery: A Case Report and Literature Review.Cureus. 2024 Feb 5;16(2):e53630. doi: 10.7759/cureus.53630. eCollection 2024 Feb. Cureus. 2024. PMID: 38449976 Free PMC article.
-
Clinical importance of the anterior choroidal artery: a review of the literature.Int J Med Sci. 2018 Feb 12;15(4):368-375. doi: 10.7150/ijms.22631. eCollection 2018. Int J Med Sci. 2018. PMID: 29511372 Free PMC article.
-
Bilateral blunt cerebrovascular injury resulting in direct carotid-cavernous fistulae: A case report and review of the literature.Surg Neurol Int. 2018 Nov 19;9:229. doi: 10.4103/sni.sni_210_18. eCollection 2018. Surg Neurol Int. 2018. PMID: 30568844 Free PMC article.
-
Endovascular treatment of blunt injury of the extracranial internal carotid artery: the prospect and dilemma.Int J Med Sci. 2021 Jan 1;18(4):944-952. doi: 10.7150/ijms.50275. eCollection 2021. Int J Med Sci. 2021. PMID: 33456352 Free PMC article. Review.
References
-
- Schievink WI, Mokri B, Whisnant JP. Internal carotid artery dissection in a community. Rochester, Minnesota, 1987–1992. Stroke 1993;24:1678–80. - PubMed
-
- Mokri B, Sundt TM Jr, Houser OW. Spontaneous internal carotid dissection, hemicrania, and Horner's syndrome. Arch Neurol 1979;36:677–80. - PubMed
-
- Leys D, Bandu L, Hénon H et al. . Clinical outcome in 287 consecutive young adults (15 to 45 years) with ischemic stroke. Neurology 2002;59:26–33. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous