

Staphylococcus aureus α-Toxin Response Distinguishes Respiratory Virus-Methicillin-Resistant S. aureus Coinfection in Children
- PMID: 27651418
- PMCID: PMC5144732
- DOI: 10.1093/infdis/jiw441
Staphylococcus aureus α-Toxin Response Distinguishes Respiratory Virus-Methicillin-Resistant S. aureus Coinfection in Children
Abstract
Background: Development of methicillin-resistant Staphylococcus aureus (MRSA) pneumonia after a respiratory viral infection is frequently fatal in children. In mice, S. aureus α-toxin directly injures pneumocytes and increases mortality, whereas α-toxin blockade mitigates disease. The role of α-toxin in pediatric staphylococcal-viral coinfection is unclear.
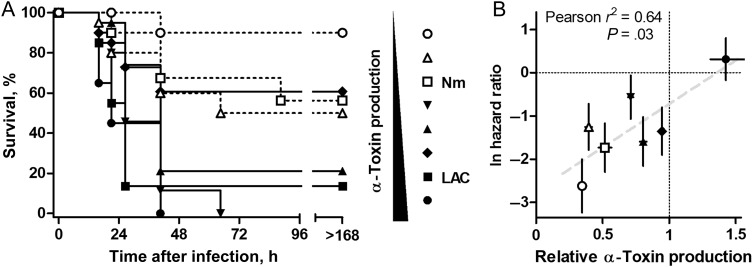
Methods: We enrolled children across 34 North American pediatric intensive care units with acute respiratory failure and suspected influenza virus infection. Serial serum anti-α-toxin antibody titers and functional α-toxin neutralization capacity were compared across children coinfected with MRSA or methicillin-susceptible S. aureus (MSSA) and control children infected with influenza virus only. MRSA isolates were tested for α-toxin production and lethality in a murine pneumonia model.
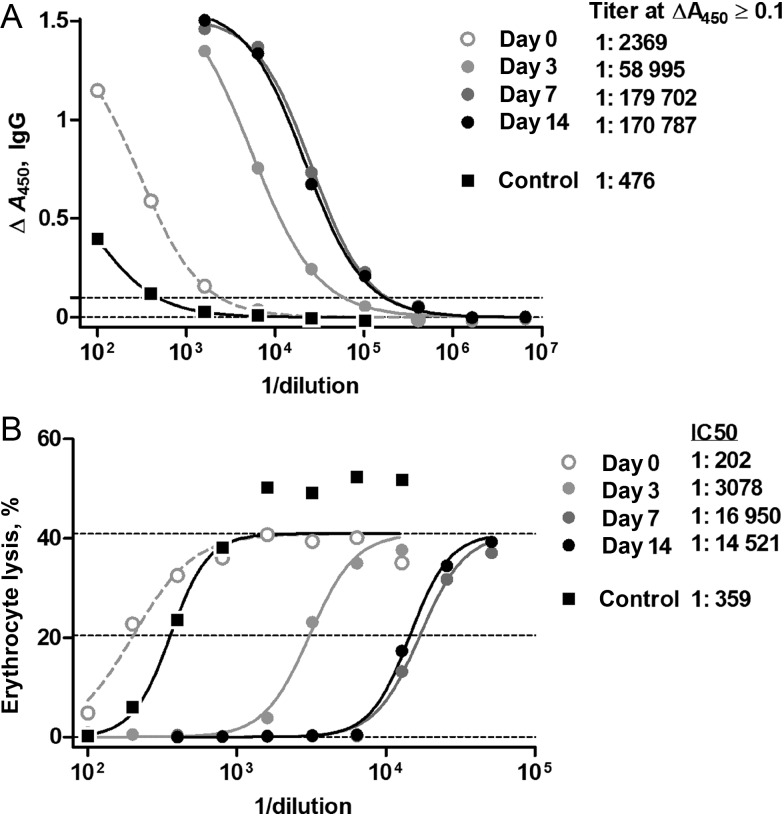
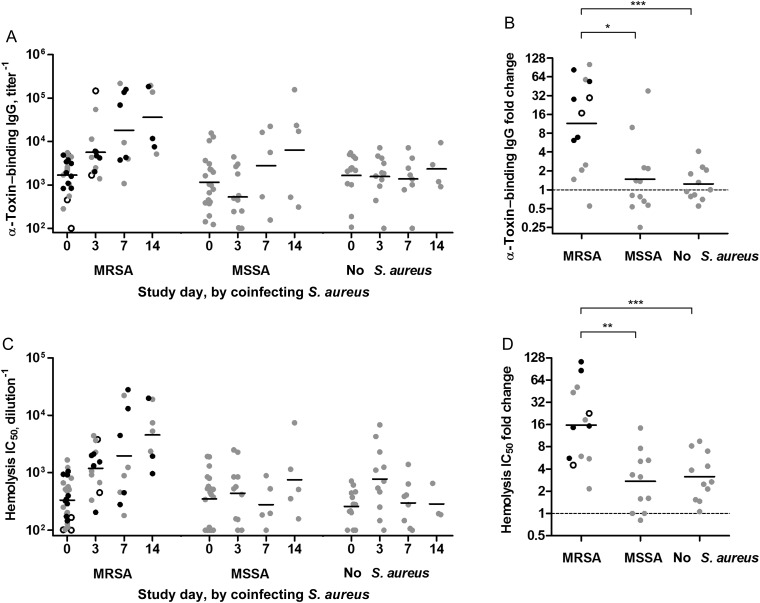
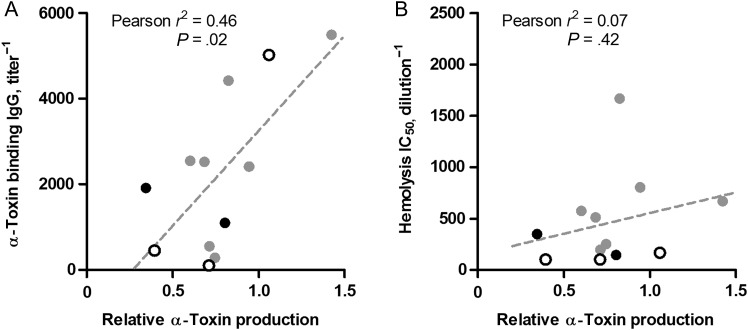
Results: Influenza virus was identified in 22 of 25 children with MRSA coinfection (9 died) and 22 patients with MSSA coinfection (all survived). Initial α-toxin-specific antibody titers were similar, compared with those in the 13 controls. In patients with serial samples, only MRSA-coinfected patients showed time-dependent increases in anti-α-toxin titer and functional neutralization capacity. MRSA α-toxin production from patient isolates correlated with initial serologic titers and with mortality in murine pneumonia.
Conclusions: These data implicate α-toxin as a relevant antigen in severe pediatric MRSA pneumonia associated with respiratory viral infection, supporting a potential role for toxin-neutralizing therapy.
Keywords: bacteria; influenza; intensive care unit; pediatric; pneumonia; respiratory failure.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
References
-
- Reed C, Kallen AJ, Patton M et al. . Infection with community-onset Staphylococcus aureus and influenza virus in hospitalized children. Pediatr Infect Dis J 2009; 28:572–6. - PubMed
-
- Finelli L, Fiore A, Dhara R et al. . Influenza-associated pediatric mortality in the United States: increase of Staphylococcus aureus coinfection. Pediatrics 2008; 122:805–11. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
