

Synergistic and Non-synergistic Associations for Cigarette Smoking and Non-tobacco Risk Factors for Cardiovascular Disease Incidence in the Atherosclerosis Risk In Communities (ARIC) Study
- PMID: 27651477
- PMCID: PMC5896551
- DOI: 10.1093/ntr/ntw235
Synergistic and Non-synergistic Associations for Cigarette Smoking and Non-tobacco Risk Factors for Cardiovascular Disease Incidence in the Atherosclerosis Risk In Communities (ARIC) Study
Abstract
Introduction: Cigarette smoking, various metabolic and lipid-related factors and hypertension are well-recognized cardiovascular disease (CVD) risk factors. Since smoking affects many of these factors, use of a single imprecise smoking metric, for example, ever or never smoked, may allow residual confounding and explain inconsistencies in current assessments of interactions.
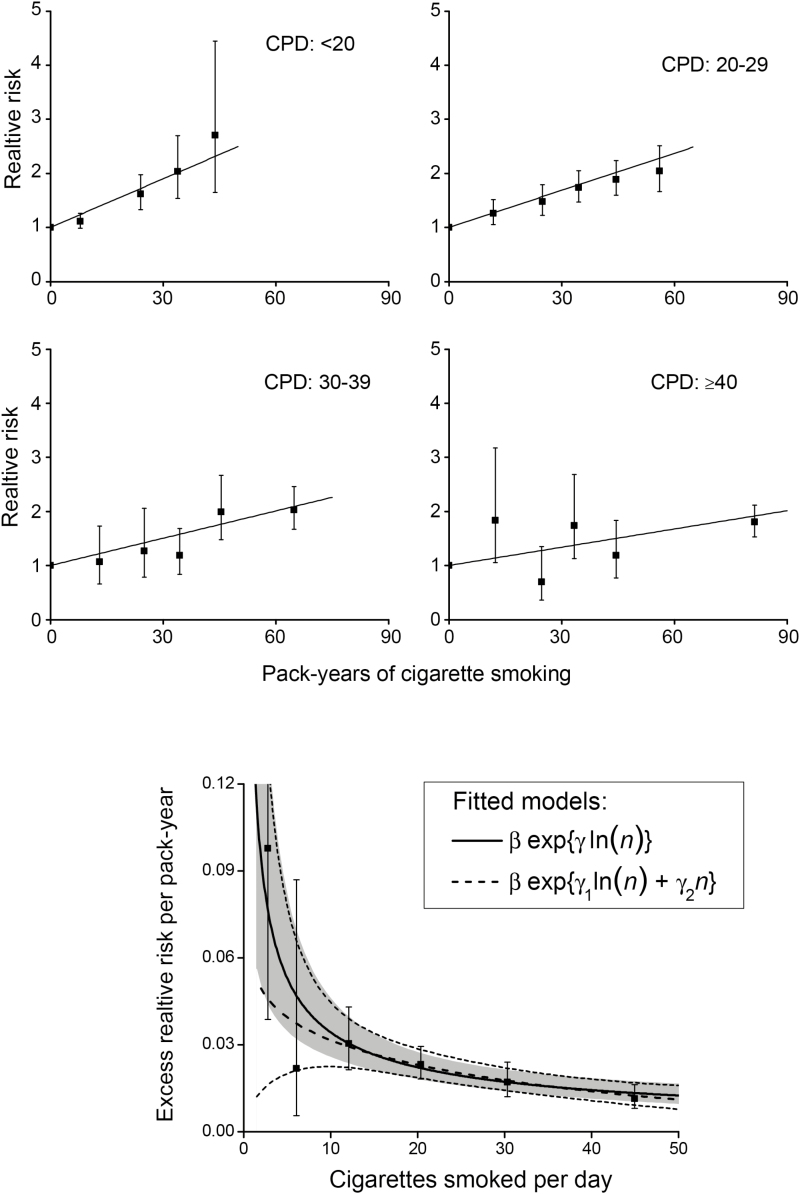
Methods: Using a comprehensive model in pack-years and cigarettes/day for the complex smoking-related relative risk (RR) of CVD to reduce residual confounding, we evaluated interactions with non-tobacco risk factors, including additive (non-synergistic) and multiplicative (synergistic) forms. Data were from the prospective Atherosclerosis Risk in Communities (ARIC) Study from four areas of the United States recruited in 1987-1989 with follow-up through 2008. Analyses included 14 127 participants, 207 693 person-years and 2857 CVD events.
Results: Analyses revealed distinct interactions with smoking: including statistical consistency with additive (body mass index [BMI], waist to hip ratio [WHR], diabetes mellitus [DM], glucose, insulin, high density lipoproteins [HDL] and HDL(2)); and multiplicative (hypertension, total cholesterol [TC], low density lipoproteins [LDLs], apolipoprotein B [apoB], TC to HDL ratio and HDL(3)) associations, as well as indeterminate (apolipoprotein A-I [apoA-I] and triglycerides) associations.
Conclusions: The forms of the interactions were revealing but require confirmation. Improved understanding of joint associations may help clarify the public health burden of smoking for CVD, links between etiologic factors and biological mechanisms, and the consequences of joint exposures, whereby synergistic associations highlight joint effects and non-synergistic associations suggest distinct contributions.
Implications: Joint associations for cigarette smoking and non-tobacco risk factors were distinct, revealing synergistic/multiplicative (hypertension, TC, LDL, apoB, TC/HDL, HDL(3)), non-synergistic/additive (BMI, WHR, DM, glucose, insulin, HDL, HDL(2)) and indeterminate (apoA-I and TRIG) associations. If confirmed, these results may help better define the public health burden of smoking on CVD risk and identify links between etiologic factors and biologic mechanisms, where synergistic associations highlight joint impacts and non-synergistic associations suggest distinct contributions from each factor.
Published by Oxford University Press on behalf of the Society for Research on Nicotine and Tobacco 2016. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
Similar articles
-
Age, Sex, and Cardiovascular Risk Attributable to Lipoprotein Cholesterol Among Chinese Individuals with Coronary Artery Disease: A Case-Control Study.Metab Syndr Relat Disord. 2019 May;17(4):223-231. doi: 10.1089/met.2018.0067. Epub 2019 Feb 5. Metab Syndr Relat Disord. 2019. PMID: 30720383
-
Risk of Cardiovascular Disease from Cumulative Cigarette Use and the Impact of Smoking Intensity.Epidemiology. 2016 May;27(3):395-404. doi: 10.1097/EDE.0000000000000437. Epidemiology. 2016. PMID: 26745609 Free PMC article.
-
Associations of lipoprotein cholesterols, apolipoproteins A-I and B, and triglycerides with carotid atherosclerosis and coronary heart disease. The Atherosclerosis Risk in Communities (ARIC) Study.Arterioscler Thromb. 1994 Jul;14(7):1098-104. doi: 10.1161/01.atv.14.7.1098. Arterioscler Thromb. 1994. PMID: 8018665
-
Molecular sources of residual cardiovascular risk, clinical signals, and innovative solutions: relationship with subclinical disease, undertreatment, and poor adherence: implications of new evidence upon optimizing cardiovascular patient outcomes.Vasc Health Risk Manag. 2013;9:617-70. doi: 10.2147/VHRM.S37119. Epub 2013 Oct 21. Vasc Health Risk Manag. 2013. PMID: 24174878 Free PMC article. Review.
-
Standardization and Prediction to Control Confounding: Estimating Risk Differences and Ratios for Clinical Interpretations and Decision Making.Ann Intern Med. 2025 Jun;178(6):829-835. doi: 10.7326/ANNALS-25-00082. Epub 2025 Apr 8. Ann Intern Med. 2025. PMID: 40194286 Review.
Cited by
-
Global burden of nasopharyngeal carcinoma attributable to alcohol use: a 1990-2021 analysis with projections to 2040.Front Public Health. 2025 Aug 7;13:1623089. doi: 10.3389/fpubh.2025.1623089. eCollection 2025. Front Public Health. 2025. PMID: 40852660 Free PMC article.
-
Incidence of Coronary Artery Disease in King Abdulaziz University Hospital, Jeddah, Saudi Arabia, 2019-2020: A Retrospective Cohort Study.Cureus. 2022 Sep 4;14(9):e28770. doi: 10.7759/cureus.28770. eCollection 2022 Sep. Cureus. 2022. PMID: 36225503 Free PMC article.
-
The Impact of 51 Risk Factors on Life Expectancy in Canada: Findings from a New Risk Prediction Model Based on Data from the Global Burden of Disease Study.Int J Environ Res Public Health. 2022 Jul 23;19(15):8958. doi: 10.3390/ijerph19158958. Int J Environ Res Public Health. 2022. PMID: 35897329 Free PMC article.
-
Cross-Sectional Gene-Smoking Interaction Analysis in Relation to Subclinical Atherosclerosis-Results From the IMPROVE Study.Circ Genom Precis Med. 2023 Jun;16(3):236-247. doi: 10.1161/CIRCGEN.122.003710. Epub 2023 Apr 6. Circ Genom Precis Med. 2023. PMID: 37021583 Free PMC article.
-
Smoking history: relationships with inflammatory markers, metabolic markers, body composition, muscle strength, and cardiopulmonary capacity in current smokers.J Bras Pneumol. 2020 Jun 15;46(5):e20180353. doi: 10.36416/1806-3756/e20180353. eCollection 2020. J Bras Pneumol. 2020. PMID: 32556029 Free PMC article.
References
-
- U.S. Department of Health and Human Services. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Washington, DC: U. S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, Superintendent of Documents, U.S. Government Printing Office; 2010. - PubMed
-
- U.S. Department of Health and Human Services. The Health Consequences of Smoking -- 50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, Superintendent of Documents, U.S. Government Printing Office; 2014.
-
- Catapano AL, Reiner Z, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Atherosclerosis. 2011;217(1):3–46. - PubMed
-
- Stone NJ, Robinson JG, Lichtenstein AH, et al. 2013 ACC/AHA Guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(25 Pt B):2889–2934. - PubMed
-
- Muscat JE, Harris RE, Haley NJ, Wynder EL. Cigarette smoking and plasma cholesterol. Am Heart J. 1991;121(1 Pt 1):141–147. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
