

Optimizing Clinical Decision Support in the Electronic Health Record. Clinical Characteristics Associated with the Use of a Decision Tool for Disposition of ED Patients with Pulmonary Embolism
- PMID: 27652375
- PMCID: PMC5052556
- DOI: 10.4338/ACI-2016-05-RA-0073
Optimizing Clinical Decision Support in the Electronic Health Record. Clinical Characteristics Associated with the Use of a Decision Tool for Disposition of ED Patients with Pulmonary Embolism
Abstract
Objective: Adoption of clinical decision support (CDS) tools by clinicians is often limited by workflow barriers. We sought to assess characteristics associated with clinician use of an electronic health record-embedded clinical decision support system (CDSS).
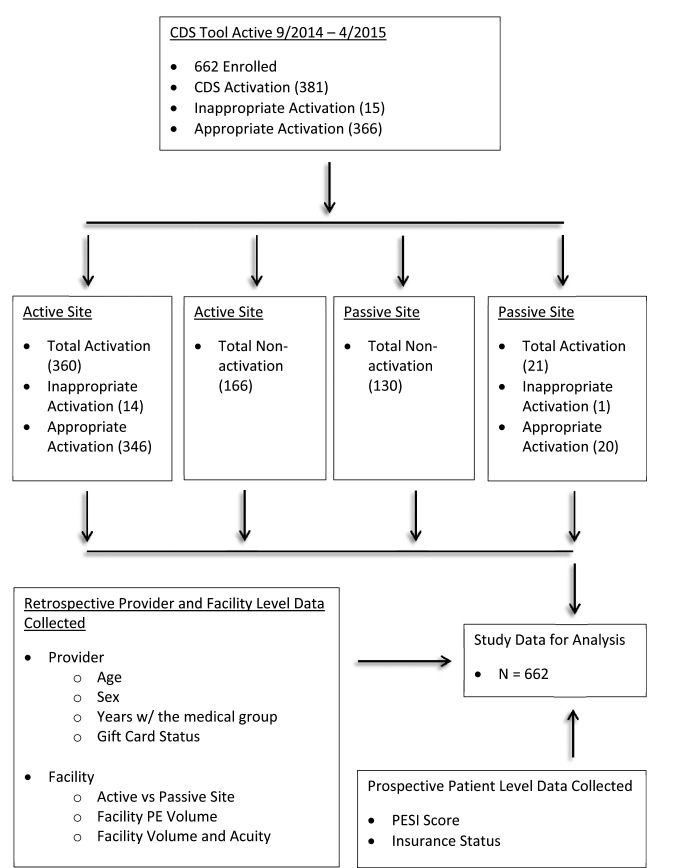
Methods: In a prospective study on emergency department (ED) activation of a CDSS tool across 14 hospitals between 9/1/14 to 4/30/15, the CDSS was deployed at 10 active sites with an on-site champion, education sessions, iterative feedback, and up to 3 gift cards/clinician as an incentive. The tool was also deployed at 4 passive sites that received only an introductory educational session. Activation of the CDSS - which calculated the Pulmonary Embolism Severity Index (PESI) score and provided guidance - and associated clinical data were collected prospectively. We used multivariable logistic regression with random effects at provider/facility levels to assess the association between activation of the CDSS tool and characteristics at: 1) patient level (PESI score), 2) provider level (demographics and clinical load at time of activation opportunity), and 3) facility level (active vs. passive site, facility ED volume, and ED acuity at time of activation opportunity).
Results: Out of 662 eligible patient encounters, the CDSS was activated in 55%: active sites: 68% (346/512); passive sites 13% (20/150). In bivariate analysis, active sites had an increase in activation rates based on the number of prior gift cards the physician had received (96% if 3 prior cards versus 60% if 0, p<0.0001). At passive sites, physicians < age 40 had higher rates of activation (p=0.03). In multivariable analysis, active site status, low ED volume at the time of diagnosis and PESI scores I or II (compared to III or higher) were associated with higher likelihood of CDSS activation.
Conclusions: Performing on-site tool promotion significantly increased odds of CDSS activation. Optimizing CDSS adoption requires active education.
Keywords: Decision-support; computerized; electronic health record; pulmonary embolism; research network.
Conflict of interest statement
The authors declare that they have no conflicts of interest in the research.
Figures
References
-
- McGlynn EA, Asch SM, Adams J, Keesey J, Hicks J, DeCristofaro A, Kerr EA. The quality of health care delivered to adults in the United States. The New England journal of medicine 2003; 348(26): 2635-2645. doi: 10.1056/NEJMsa022615. PubMed PMID: 12826639. - PubMed
-
- Balas EA, Boren SA. Managing clinical knowledge for health care improvement. Yearbook of Medical Informatics 2000; 65(70). - PubMed
-
- Davidoff F. On the undiffusion of established practices. JAMA internal medicine 2015; 175(5): 809-811. doi: 10.1001/jamainternmed.2015.0167. PubMed PMID: 25774743. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
