

doi: 10.1097/IMI.0000000000000300.
Minimally Invasive Mitral Valve Surgery II: Surgical Technique and Postoperative Management
Affiliations
- PMID: 27654406
- PMCID: PMC5051532
- DOI: 10.1097/IMI.0000000000000300
Item in Clipboard
Minimally Invasive Mitral Valve Surgery II: Surgical Technique and Postoperative Management
Innovations (Phila).
2016 Jul-Aug.
Abstract
Techniques for minimally invasive mitral valve repair and replacement continue to evolve. This expert opinion, the second of a 3-part series, outlines current best practices for nonrobotic, minimally invasive mitral valve procedures, and for postoperative care after minimally invasive mitral valve surgery.
Figures
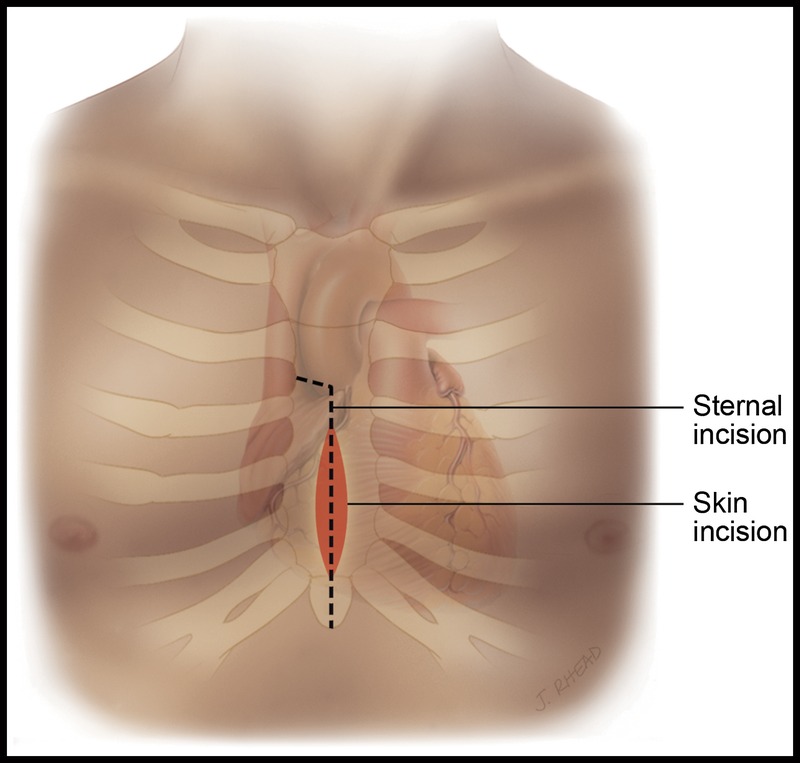
Lower hemisternotomy incision.
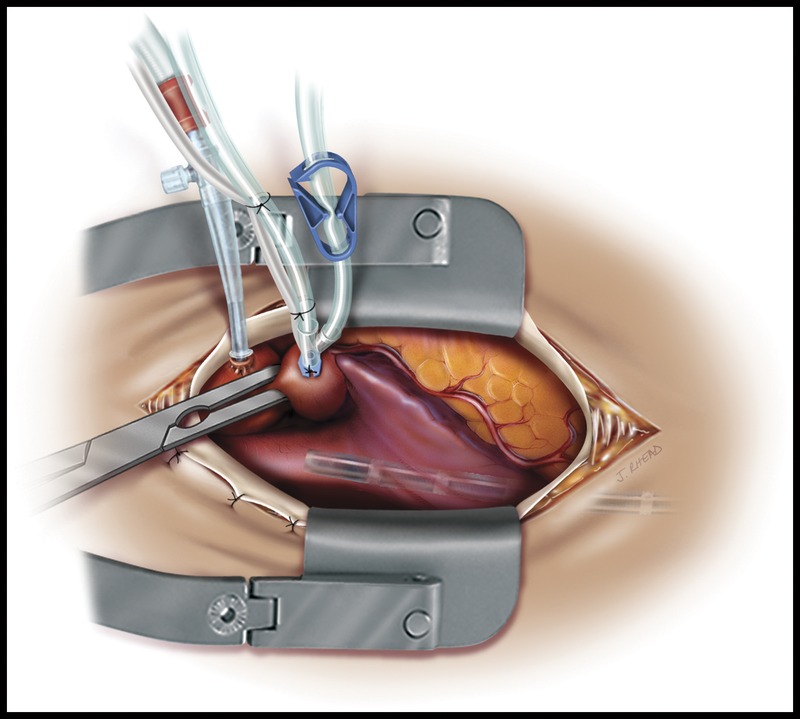
Lower hemisternotomy showing placement of retractor and cannulae.
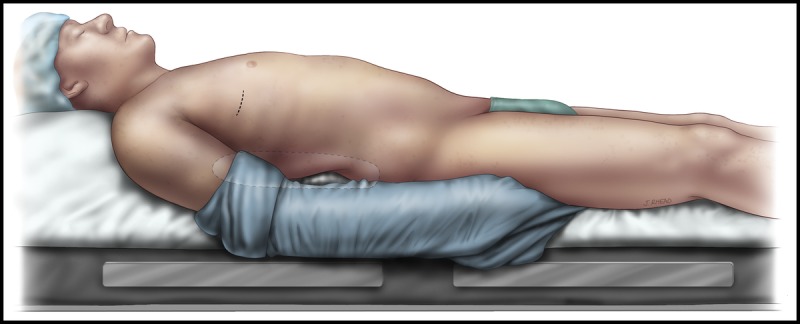
Patient positioning for direct-vision right minithoracotomy, showing a small pillow placed inferior to the scapula (transparent ellipse). The vertical dashed line indicates the placement of the primary incision.
Exteriorization of sutures for diaphragmatic retraction.
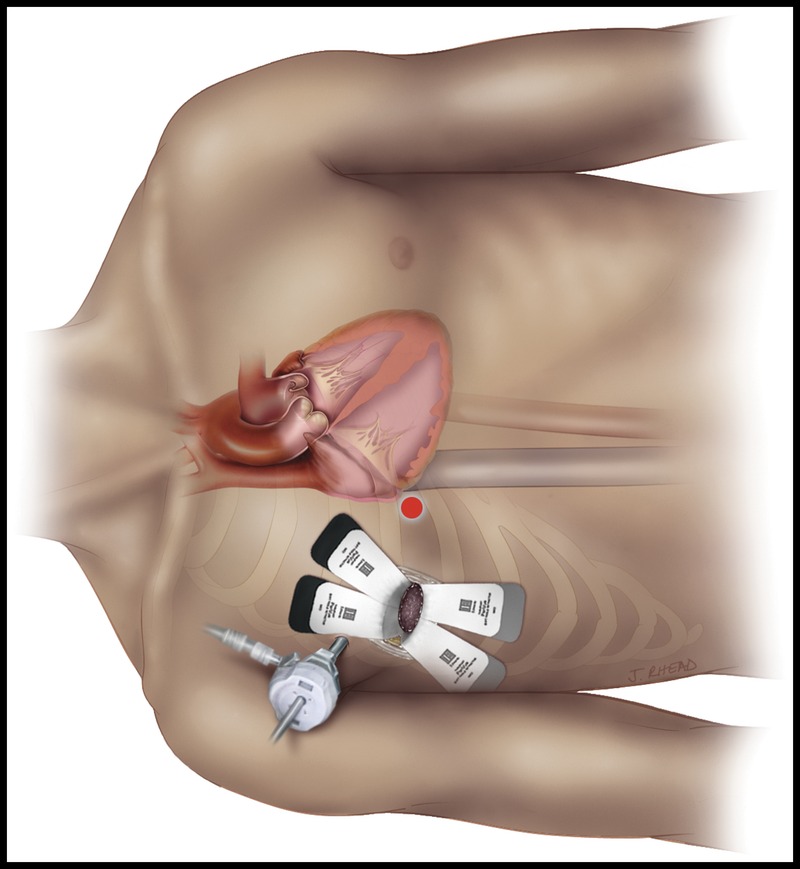
Incisions for working port and retractor. The red dot represents the location of the incision for the retractor.
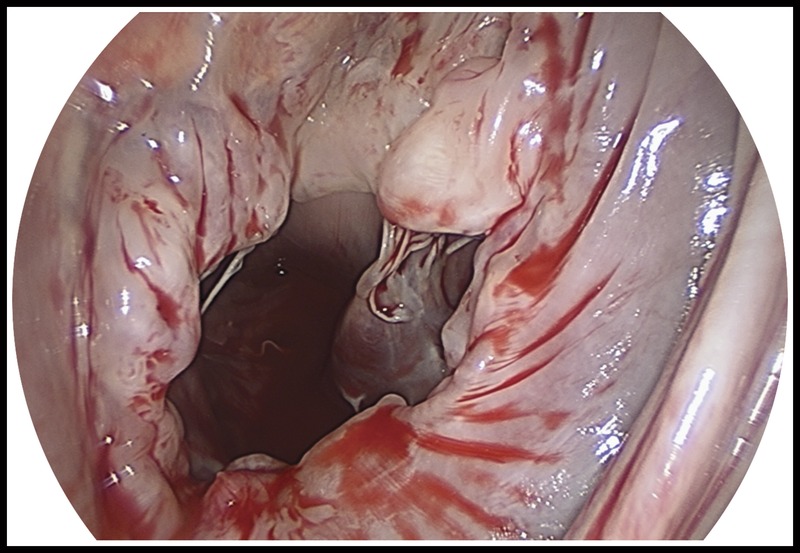
Retraction of the interatrial septum.
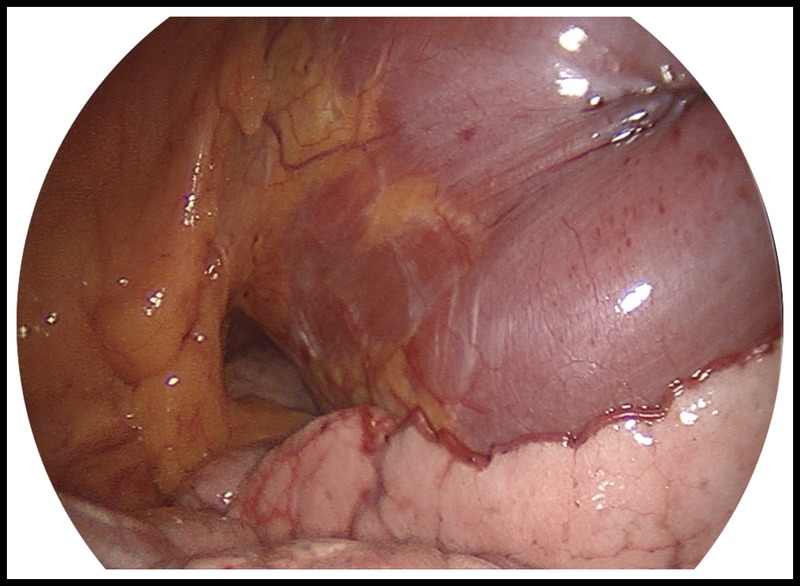
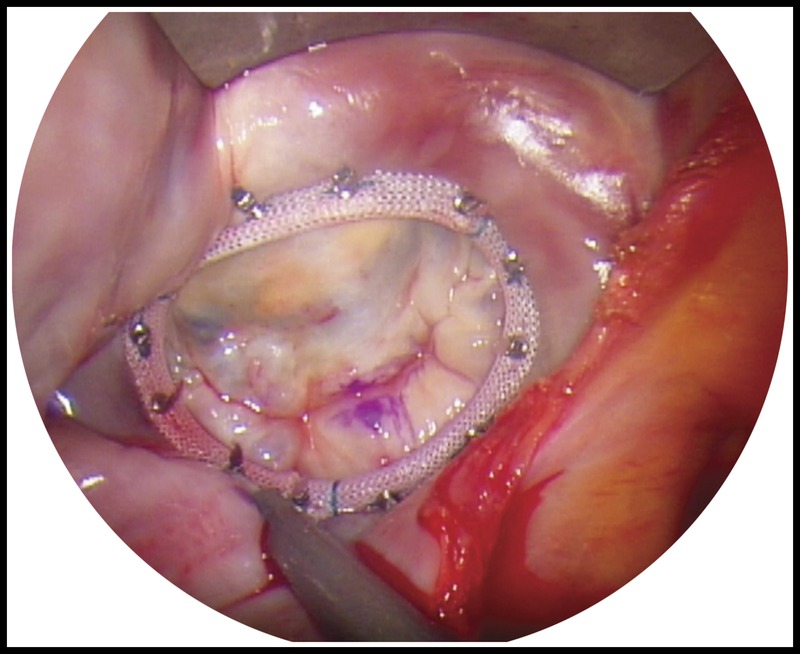
Endoscopic visualization of the MV.
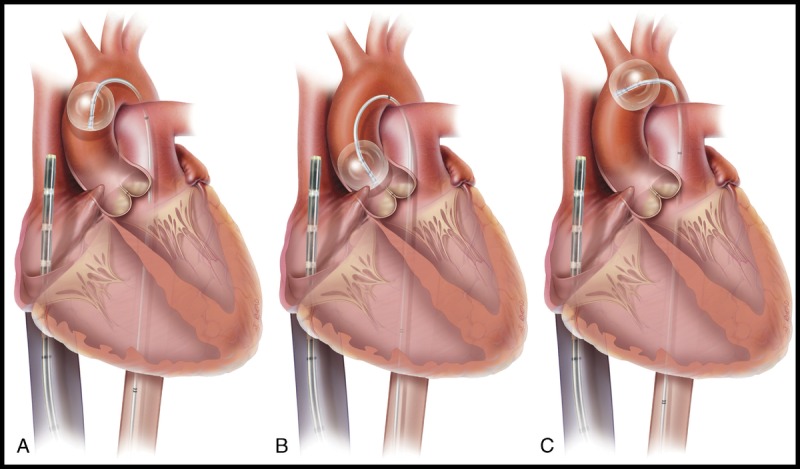
Endoaortic occlusion balloon positioning. A, Correct balloon position. B, Proximal migration may allow leakage around the balloon and possible iatrogenic puncture. C, Distal migration may diminish brachiocephalic perfusion. Note the tip of the venous cannula 2 to 3 cm above the junction of the right atrium and superior vena cava.
References
-
- Youssef SJ, Millan JA, Youssef GM, Earnheart A, Lehr EJ, Barnhart GR. The role of computed tomography angiography in patients undergoing evaluation for minimally invasive cardiac surgery: an early program experience. Innovations. 2015;10:33–38. - PubMed
-
- Rodriguez R, Gojkovic O, Khitri A, et al. Totally endoscopic minimally invasive mitral valve surgery as a routine approach: a 10 year experience. Mitral Conclave American Association for Thoracic Surgery, Sheraton Towers, New York, NY USA, May 5–6, 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
