

Cellular and Morphological Alterations in the Vastus Lateralis Muscle as the Result of ACL Injury and Reconstruction
- PMID: 27655981
- PMCID: PMC5026157
- DOI: 10.2106/JBJS.16.00035
Cellular and Morphological Alterations in the Vastus Lateralis Muscle as the Result of ACL Injury and Reconstruction
Abstract
Background: Individuals who have had an anterior cruciate ligament (ACL) tear and reconstruction continue to experience substantial knee extensor strength loss despite months of physical therapy. Identification of the alterations in muscle morphology and cellular composition are needed to understand potential mechanisms of muscle strength loss, initially as the result of the injury and subsequently from surgery and rehabilitation.
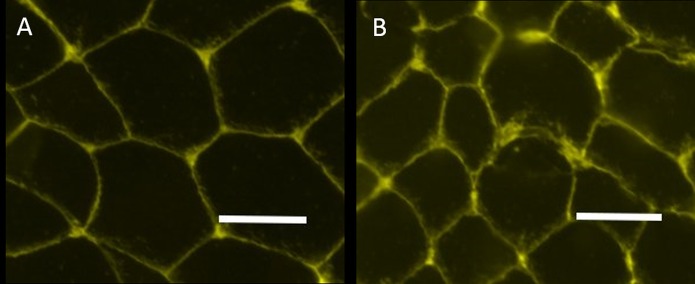
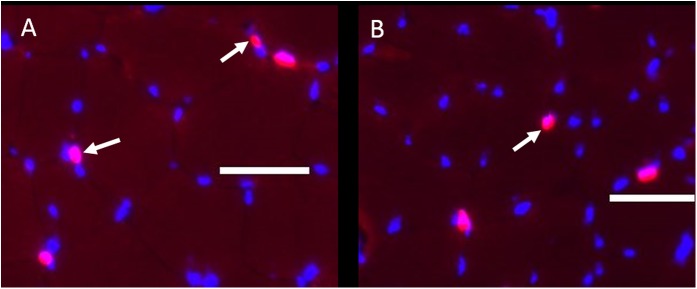
Methods: We performed diffusion tensor imaging-magnetic resonance imaging and analyzed muscle biopsies from the vastus lateralis of both the affected and unaffected limbs before surgery and again from the reconstructed limb following the completion of rehabilitation. Immunohistochemistry was done to determine fiber type and size, Pax-7-positive (satellite) cells, and extracellular matrix (via wheat germ agglutinin straining). Using the diffusion tensor imaging data, the fiber tract length, pennation angle, and muscle volume were determined, yielding the physiological cross-sectional area (PCSA). Paired t tests were used to compare the effects of the injury between injured and uninjured limbs and the effects of surgery and rehabilitation within the injured limb.
Results: We found significant reductions before surgery in type-IIA muscle cross-sectional area (CSA; p = 0.03), extracellular matrix (p < 0.01), satellite cells per fiber (p < 0.01), pennation angle (p = 0.03), muscle volume (p = 0.02), and PCSA (p = 0.03) in the injured limb compared with the uninjured limb. Following surgery, these alterations in the injured limb persisted and the frequency of the IIA fiber type decreased significantly (p < 0.01) and that of the IIA/X hybrid fiber type increased significantly (p < 0.01).
Conclusions: Significant and prolonged differences in muscle quality and morphology occurred after ACL injury and persisted despite reconstruction and extensive physical therapy.
Clinical relevance: These results suggest the need to develop more effective early interventions following an ACL tear to prevent deleterious alterations within the quadriceps.
Copyright © 2016 by The Journal of Bone and Joint Surgery, Incorporated.
Figures

Comment in
-
What Happened to My Quad? Commentary on an article by Brian Noehren, PT, PhD, et al.: "Cellular and Morphological Alterations in the Vastus Lateralis Muscle as the Result of ACL Injury and Reconstruction".J Bone Joint Surg Am. 2016 Sep 21;98(18):e79. doi: 10.2106/JBJS.16.00635. J Bone Joint Surg Am. 2016. PMID: 27655991 No abstract available.
References
-
- Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M, Dick RW, Engebretsen L, Garrett WE Jr, Hannafin JA, Hewett TE, Huston LJ, Ireland ML, Johnson RJ, Lephart S, Mandelbaum BR, Mann BJ, Marks PH, Marshall SW, Myklebust G, Noyes FR, Powers C, Shields C Jr, Shultz SJ, Silvers H, Slauterbeck J, Taylor DC, Teitz CC, Wojtys EM, Yu B. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med. 2006. September;34(9):1512-32. - PubMed
-
- McLean SG, Beaulieu ML. Complex integrative morphological and mechanical contributions to ACL injury risk. Exerc Sport Sci Rev. 2010. October;38(4):192-200. - PubMed
-
- Hiemstra LA, Webber S, MacDonald PB, Kriellaars DJ. Knee strength deficits after hamstring tendon and patellar tendon anterior cruciate ligament reconstruction. Med Sci Sports Exerc. 2000. August;32(8):1472-9. - PubMed
-
- DeVita P, Hortobagyi T, Barrier J. Gait biomechanics are not normal after anterior cruciate ligament reconstruction and accelerated rehabilitation. Med Sci Sports Exerc. 1998. October;30(10):1481-8. - PubMed
-
- Paterno MV, Ford KR, Myer GD, Heyl R, Hewett TE. Limb asymmetries in landing and jumping 2 years following anterior cruciate ligament reconstruction. Clin J Sport Med. 2007. July;17(4):258-62. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
