

Cystic and Papillary Neoplasm at the Hepatic Hilum Possibly Originating in the Peribiliary Glands
- PMID: 27656307
- PMCID: PMC5021872
- DOI: 10.1155/2016/9130754
Cystic and Papillary Neoplasm at the Hepatic Hilum Possibly Originating in the Peribiliary Glands
Abstract
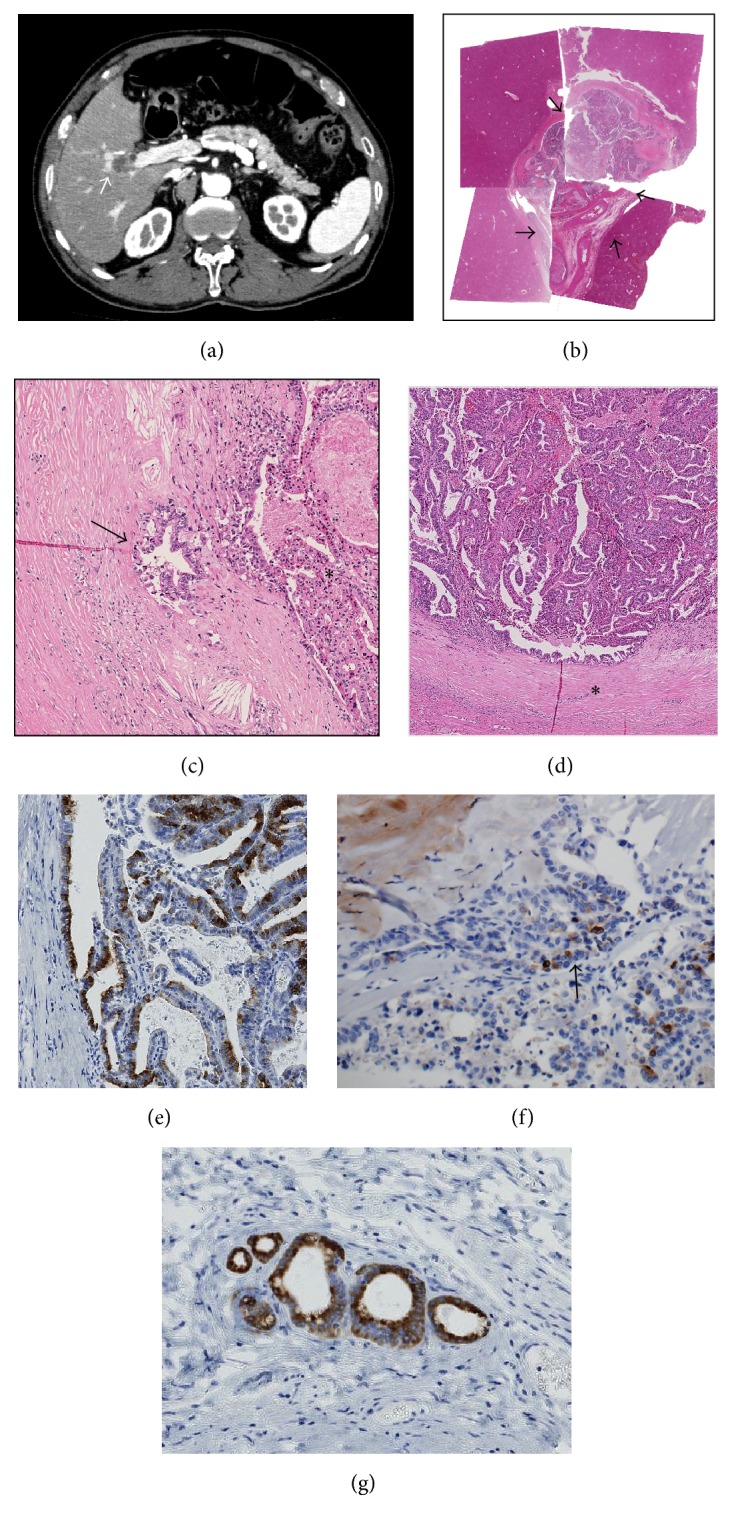
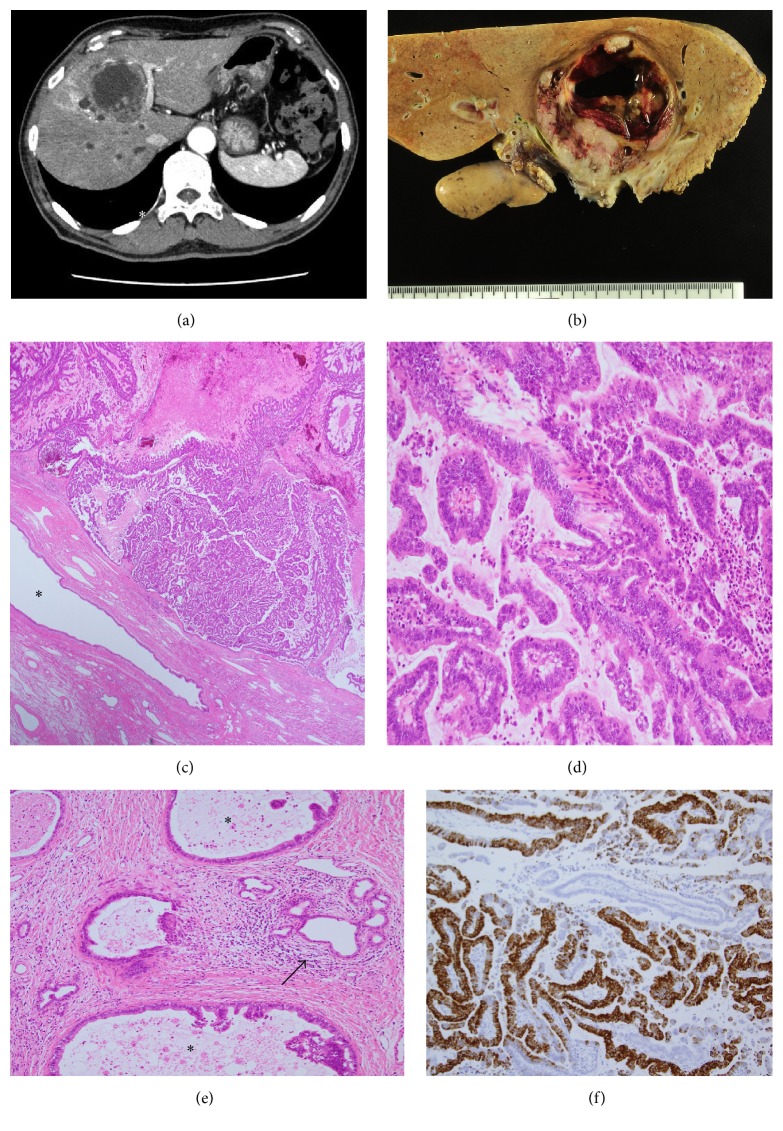
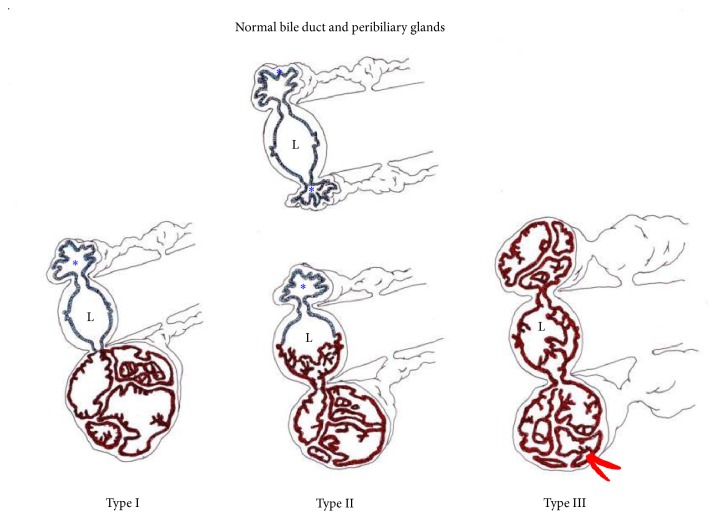
Cystic neoplasms of the liver are divided into two types: mucinous cystic neoplasm and cystic intraductal papillary neoplasm of the bile duct. We herein report two cases of cystic and papillary neoplasm of the liver which differed from the abovementioned types. Case 1. A 70-year-old man. Radiologically, a cystic tumor measuring 20 mm in diameter was found at the hepatic hilum. Right hepatectomy was performed under a diagnosis of intrahepatic cholangiocarcinoma (iCCA) based on the imaging findings. Case 2. A 70-year-old man. Radiologically, a cystic tumor measuring 60 mm in diameter was found at the hepatic hilum. Under a diagnosis of iCCA, left hepatic trisectionectomy was performed. In both cases, endoscopic retrograde cholangiography did not demonstrate communication between the cystic tumor and adjacent bile ducts. Pathologically, these two tumors were cystic neoplasms located at the hepatic hilum and were morphologically characterized by an intracystic papillary neoplasm composed of diffuse high-grade dysplasia and associated with an invasive carcinoma. Ovarian-like stroma was not found in the capsule of these tumors. Interestingly, there were peribiliary glands near these tumors, and MUC6 was expressed in these papillary neoplasms as well as in the peribiliary glands. These neoplasms might have arisen from the peribiliary glands.
Figures
References
-
- Nakanuma Y., Curabo M. O., Franceschi S., et al. WHO Classification of Tumours of the Digestive System World Health Organization Classification of Tumours. 4th. chapter 10. Lyon, France: IARC Press; 2010. Intrahepatic cholangiocarcinoma; pp. 217–224.
-
- Tsui W. M. S., Adsay N. V., Crawford J. M., Hruban R., Kloppel G., Wee A. Mucinous cystic neoplasms of the liver. In: Bosman F. T., Carneiro F., Hruban R. H., Theise N. D., editors. World Health Organization Classification of Tumours. Pathology and Genetics of Tumours of the Digestive System. 4th. chapter 10. Lyon, France: IARC Press; 2010. pp. 236–238.
-
- Chen T. C., Nakanuma Y., Zen Y., et al. Intraductal papillary neoplasia of the liver associated with hepatolithiasis. Hepatology. 2001;44(5):1333–1343. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
