

A Fluoroscopy-Free Technique for Percutaneous Screw Positioning During Arthroscopic Treatment of Depression Tibial Plateau Fractures
- PMID: 27656370
- PMCID: PMC5021518
- DOI: 10.1016/j.eats.2016.02.012
A Fluoroscopy-Free Technique for Percutaneous Screw Positioning During Arthroscopic Treatment of Depression Tibial Plateau Fractures
Abstract
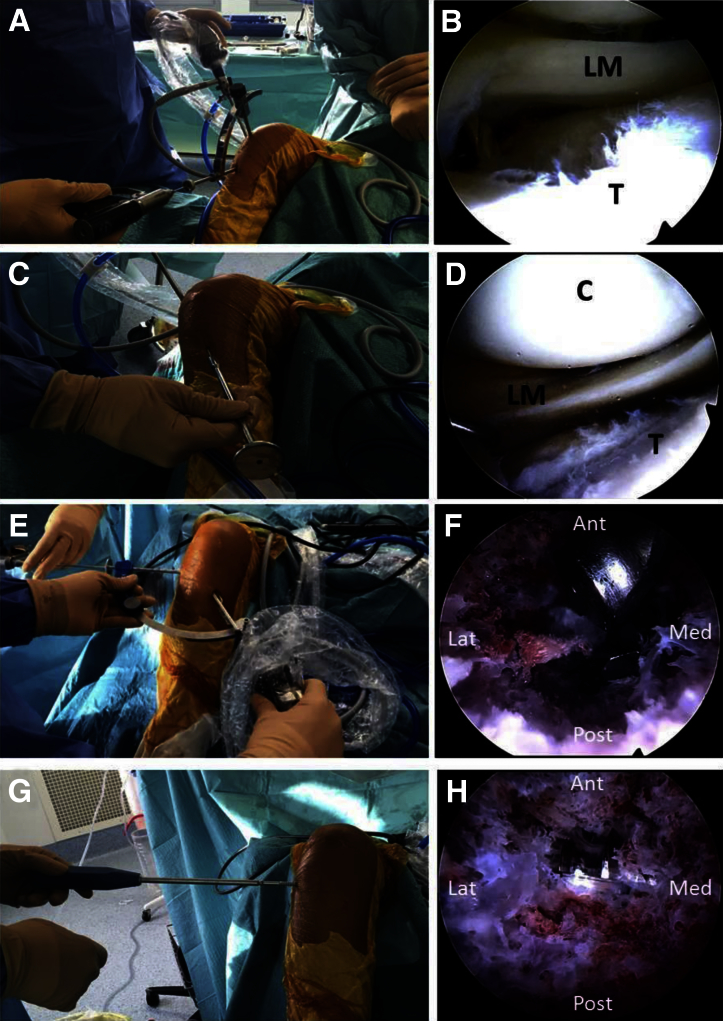
This article aims to describe a simple and reliable technique that helps in positioning the cannulated percutaneous screws during fixation of depression-type tibial plateau fractures. After fracture reduction under arthroscopic control, an outside-in anterior cruciate ligament femoral guide is introduced through the tibial cortical metaphyseal window and positioned under endoscopic control just underneath the elevated fragment. When proper height is achieved, a guide pin is drilled from lateral to medial through the sleeve, 1 to 2 cm distal to the articular surface of the depressed fragment. The cannulated screw can then be introduced under endoscopic control, without fluoroscopic assistance, just under the previously elevated joint surface. This technique ensures optimal placement of the cannulated screw in the middle of the bony tunnel to obtain optimal subchondral bone support during fixation of the depressed tibial plateau fracture.
Figures


References
-
- Caspari R.B., Hutton P.M., Whipple T.L., Meyers J.F. The role of arthroscopy in the management of tibial plateau fractures. Arthroscopy. 1985;1:76–82. - PubMed
-
- Jennings J.E. Arthroscopic management of tibial plateau fractures. Arthroscopy. 1985;1:160–168. - PubMed
-
- Burdin G. Arthroscopic management of tibial plateau fractures: Surgical technique. Orthop Traumatol Surg Res. 2013;99(suppl):S208–S218. - PubMed
-
- Suganuma J., Akutsu S. Arthroscopically assisted treatment of tibial plateau fractures. Arthroscopy. 2004;20:1084–1089. - PubMed
-
- Lubowitz J.H., Elson W.S., Guttmann D. Part I: Arthroscopic management of tibial plateau fractures. Arthroscopy. 2004;20:1063–1070. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
