

Differential Impact of Hyperglycemia in Critically Ill Patients: Significance in Acute Myocardial Infarction but Not in Sepsis?
- PMID: 27657056
- PMCID: PMC5037851
- DOI: 10.3390/ijms17091586
Differential Impact of Hyperglycemia in Critically Ill Patients: Significance in Acute Myocardial Infarction but Not in Sepsis?
Abstract
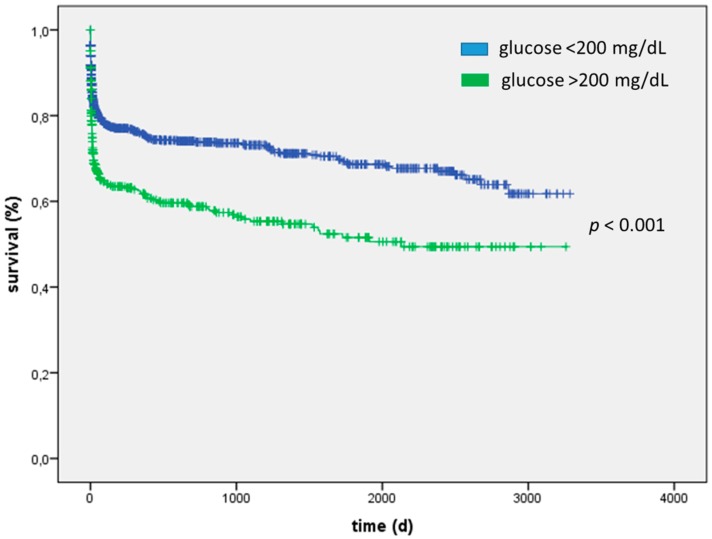
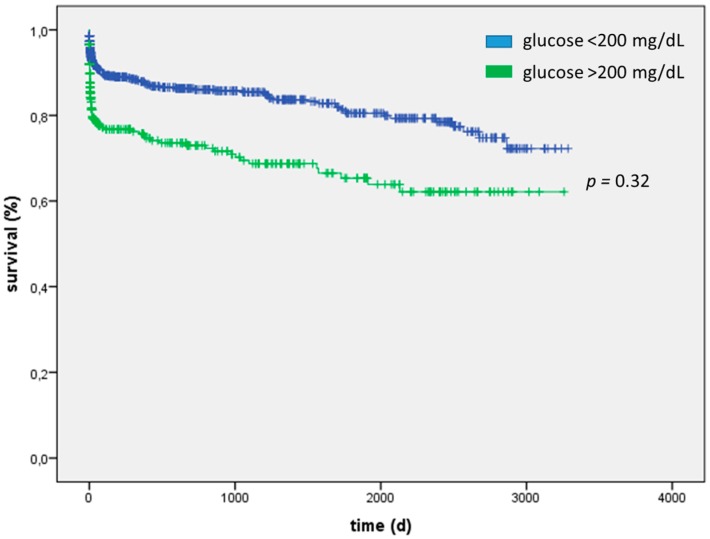
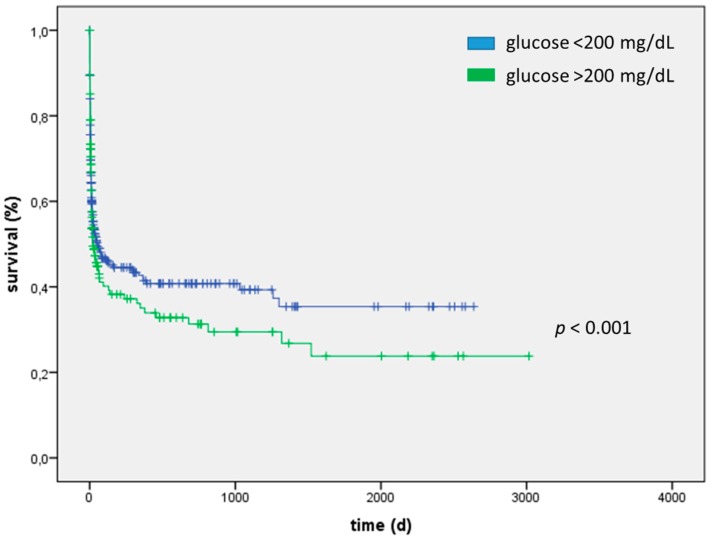
Hyperglycemia is a common condition in critically ill patients admitted to an intensive care unit (ICU). These patients represent an inhomogeneous collective and hyperglycemia might need different evaluation depending on the underlying disorder. To elucidate this, we investigated and compared associations of severe hyperglycemia (>200 mg/dL) and mortality in patients admitted to an ICU for acute myocardial infarction (AMI) or sepsis as the two most frequent admission diagnoses. From 2006 to 2009, 2551 patients 69 (58-77) years; 1544 male; 337 patients suffering from type 2 diabetes (T2DM)) who were admitted because of either AMI or sepsis to an ICU in a tertiary care hospital were investigated retrospectively. Follow-up of patients was performed between May 2013 and November 2013. In a Cox regression analysis, maximum glucose concentration at the day of admission was associated with mortality in the overall cohort (HR = 1.006, 95% CI: 1.004-1.009; p < 0.001) and in patients suffering from myocardial infarction (HR = 1.101, 95% CI: 1.075-1.127; p < 0.001) but only in trend in patients admitted to an ICU for sepsis (HR = 1.030, 95% CI: 0.998-1.062; p = 0.07). Severe hyperglycemia was associated with adverse intra-ICU mortality in the overall cohort (23% vs. 13%; p < 0.001) and patients admitted for AMI (15% vs. 5%; p < 0.001) but not for septic patients (39% vs. 40%; p = 0.48). A medical history of type 2 diabetes (n = 337; 13%) was not associated with increased intra-ICU mortality (15% vs. 15%; p = 0.93) but in patients with severe hyperglycemia and/or a known medical history of type 2 diabetes considered in combination, an increased mortality in AMI patients (intra-ICU 5% vs. 13%; p < 0.001) but not in septic patients (intra-ICU 38% vs. 41%; p = 0.53) could be evidenced. The presence of hyperglycemia in critically ill patients has differential impact within the different etiological groups. Hyperglycemia in AMI patients might identify a sicker patient collective suffering from pre-diabetes or undiagnosed diabetes with its' known adverse consequences, especially in the long-term. Hyperglycemia in sepsis might be considered as adaptive survival mechanism to hypo-perfusion and consecutive lack of glucose in peripheral cells. AMI patients with hyperglycemic derailment during an ICU-stay should be closely followed-up and extensively screened for diabetes to improve patients' outcome.
Keywords: critically ill; diabetes; hyperglycemia; myocardial infarction; prediabetes; sepsis; stress hyperglycemia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Hoebers L.P., Damman P., Claessen B.E., Vis M.M., Baan J., Jr., van Straalen J.P., Fischer J., Koch K.T., Tijssen J.G., de Winter R.J., et al. Predictive value of plasma glucose level on admission for short and long term mortality in patients with ST-elevation myocardial infarction treated with primary percutaneous coronary intervention. Am. J. Cardiol. 2012;109:53–59. doi: 10.1016/j.amjcard.2011.07.067. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
