

Beyond Risk Compensation: Clusters of Antiretroviral Treatment (ART) Users in Sexual Networks Can Modify the Impact of ART on HIV Incidence
- PMID: 27657492
- PMCID: PMC5033240
- DOI: 10.1371/journal.pone.0163159
Beyond Risk Compensation: Clusters of Antiretroviral Treatment (ART) Users in Sexual Networks Can Modify the Impact of ART on HIV Incidence
Abstract
Introduction: Concerns about risk compensation-increased risk behaviours in response to a perception of reduced HIV transmission risk-after the initiation of ART have largely been dispelled in empirical studies, but other changes in sexual networking patterns may still modify the effects of ART on HIV incidence.
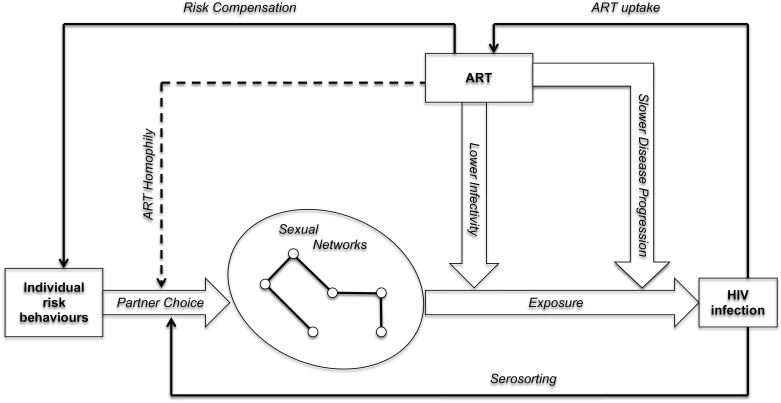
Methods: We developed an exploratory mathematical model of HIV transmission that incorporates the possibility of ART clusters, i.e. subsets of the sexual network in which the density of ART patients is much higher than in the rest of the network. Such clusters may emerge as a result of ART homophily-a tendency for ART patients to preferentially form and maintain relationships with other ART patients. We assessed whether ART clusters may affect the impact of ART on HIV incidence, and how the influence of this effect-modifying variable depends on contextual variables such as HIV prevalence, HIV serosorting, coverage of HIV testing and ART, and adherence to ART.
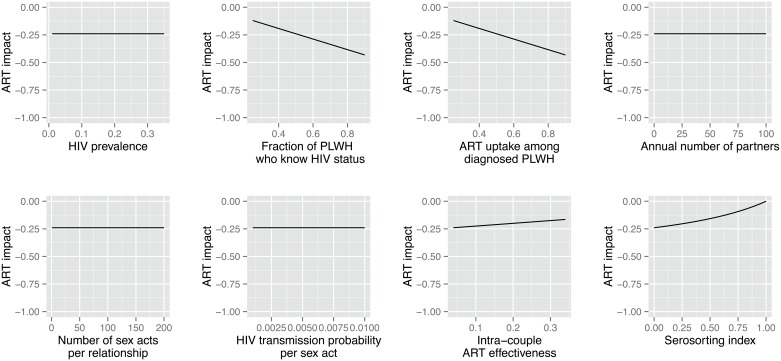
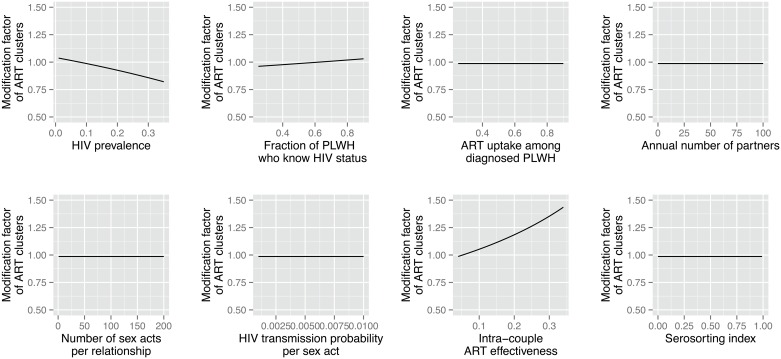
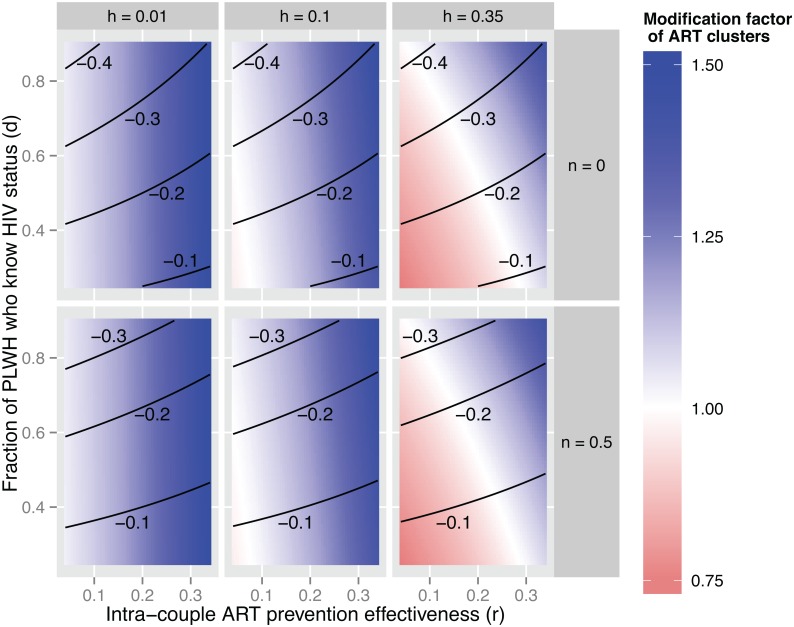
Results: ART homophily can modify the impact of ART on HIV incidence in both directions. In concentrated epidemics and generalized epidemics with moderate HIV prevalence (≈ 10%), ART clusters can enhance the impact of ART on HIV incidence, especially when adherence to ART is poor. In hyperendemic settings (≈ 35% HIV prevalence), ART clusters can reduce the impact of ART on HIV incidence when adherence to ART is high but few people living with HIV (PLWH) have been diagnosed. In all contexts, the effects of ART clusters on HIV epidemic dynamics are distinct from those of HIV serosorting.
Conclusions: Depending on the programmatic and epidemiological context, ART clusters may enhance or reduce the impact of ART on HIV incidence, in contrast to serosorting, which always leads to a lower impact of ART on HIV incidence. ART homophily and the emergence of ART clusters should be measured empirically and incorporated into more refined models used to plan and evaluate ART programmes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
Changes in the transmission dynamics of the HIV epidemic after the wide-scale use of antiretroviral therapy could explain increases in sexually transmitted infections: results from mathematical models.Sex Transm Dis. 2004 Feb;31(2):100-13. doi: 10.1097/01.OLQ.0000112721.21285.A2. Sex Transm Dis. 2004. PMID: 14743073
-
Population-level impact of an accelerated HIV response plan to reach the UNAIDS 90-90-90 target in Côte d'Ivoire: Insights from mathematical modeling.PLoS Med. 2017 Jun 15;14(6):e1002321. doi: 10.1371/journal.pmed.1002321. eCollection 2017 Jun. PLoS Med. 2017. PMID: 28617810 Free PMC article.
-
The impact of the transmission dynamics of the HIV/AIDS epidemic on sexual behaviour: a new hypothesis to explain recent increases in risk taking-behaviour among men who have sex with men.Med Hypotheses. 2005;65(2):215-26. doi: 10.1016/j.mehy.2005.03.017. Med Hypotheses. 2005. PMID: 15922091
-
Review: [corrected] The changing face of the HIV epidemic in sub-Saharan Africa.Trop Med Int Health. 2014 Sep;19(9):1015-28. doi: 10.1111/tmi.12344. Epub 2014 Jun 27. Trop Med Int Health. 2014. PMID: 24976370 Review.
-
AIDS in sub-Saharan Africa: the epidemiology of heterosexual transmission and the prospects for prevention.Epidemiology. 1993 Jan;4(1):63-72. Epidemiology. 1993. PMID: 8420583 Review.
Cited by
-
Population-Level Sexual Mixing According to HIV Status and Preexposure Prophylaxis Use Among Men Who Have Sex With Men in Montreal, Canada: Implications for HIV Prevention.Am J Epidemiol. 2020 Jan 31;189(1):44-54. doi: 10.1093/aje/kwz231. Am J Epidemiol. 2020. PMID: 31612213 Free PMC article.
-
HIV seroconcordance among heterosexual couples in rural KwaZulu-Natal, South Africa: a population-based analysis.J Int AIDS Soc. 2020 Jan;23(1):e25432. doi: 10.1002/jia2.25432. J Int AIDS Soc. 2020. PMID: 31916420 Free PMC article.
-
Is There Risk Compensation among HIV Infected Youth and Adults 15 Years and Older on Antiretroviral Treatment in South Africa? Findings from the 2017 National HIV Prevalence, Incidence, Behaviour and Communication Survey.Int J Environ Res Public Health. 2022 May 18;19(10):6156. doi: 10.3390/ijerph19106156. Int J Environ Res Public Health. 2022. PMID: 35627693 Free PMC article.
-
No effect of test and treat on sexual behaviours at population level in rural South Africa.AIDS. 2019 Mar 15;33(4):709-722. doi: 10.1097/QAD.0000000000002104. AIDS. 2019. PMID: 30608273 Free PMC article.
-
Effect of population viral load on prospective HIV incidence in a hyperendemic rural African community.Sci Transl Med. 2017 Dec 13;9(420):eaam8012. doi: 10.1126/scitranslmed.aam8012. Sci Transl Med. 2017. PMID: 29237762 Free PMC article.
References
-
- Jean K, Gabillard D, Moh R, Danel C, Fassassi R, Desgrees-du-Lou A, et al. Effect of Early Antiretroviral Therapy on Sexual Behaviors and HIV-1 Transmission Risk Among Adults With Diverse Heterosexual Partnership Statuses in Cote d'Ivoire. J Infect Dis 2014,209:431–440. 10.1093/infdis/jit470 - DOI - PMC - PubMed
-
- Grinsztejn B, Hosseinipour MC, Ribaudo HJ, Swindells S, Eron J, Chen YQ, et al. Effects of early versus delayed initiation of antiretroviral treatment on clinical outcomes of HIV-1 infection: results from the phase 3 HPTN 052 randomised controlled trial. Lancet Infect Dis 2014,14:281–290. 10.1016/S1473-3099(13)70692-3 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
