

Comparison of spoiled gradient echo and steady-state free-precession imaging for native myocardial T1 mapping using the slice-interleaved T1 mapping (STONE) sequence
- PMID: 27658506
- PMCID: PMC5599252
- DOI: 10.1002/nbm.3598
Comparison of spoiled gradient echo and steady-state free-precession imaging for native myocardial T1 mapping using the slice-interleaved T1 mapping (STONE) sequence
Abstract
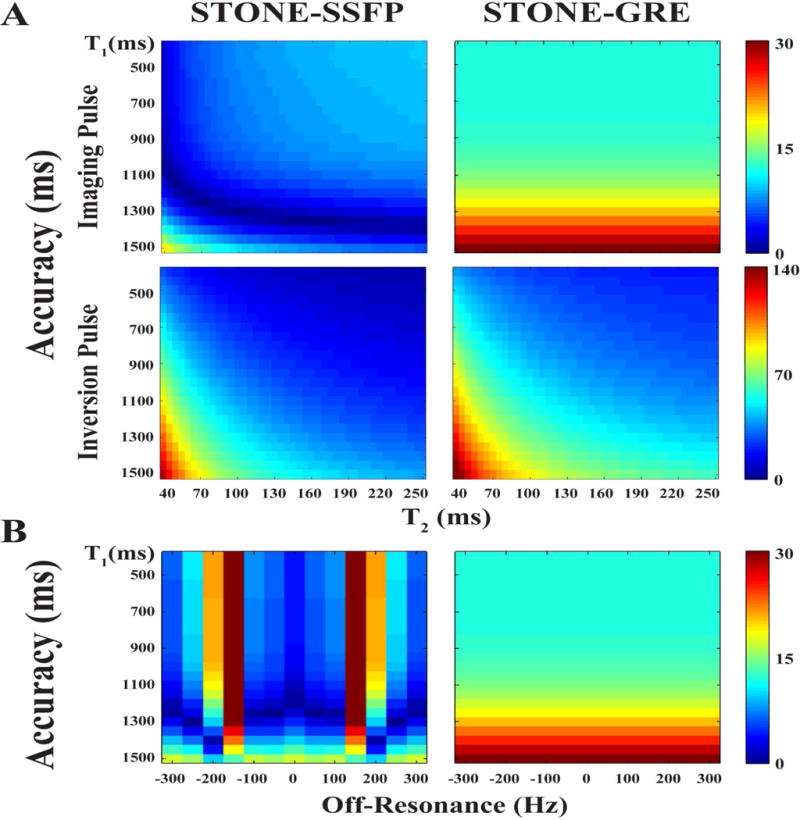
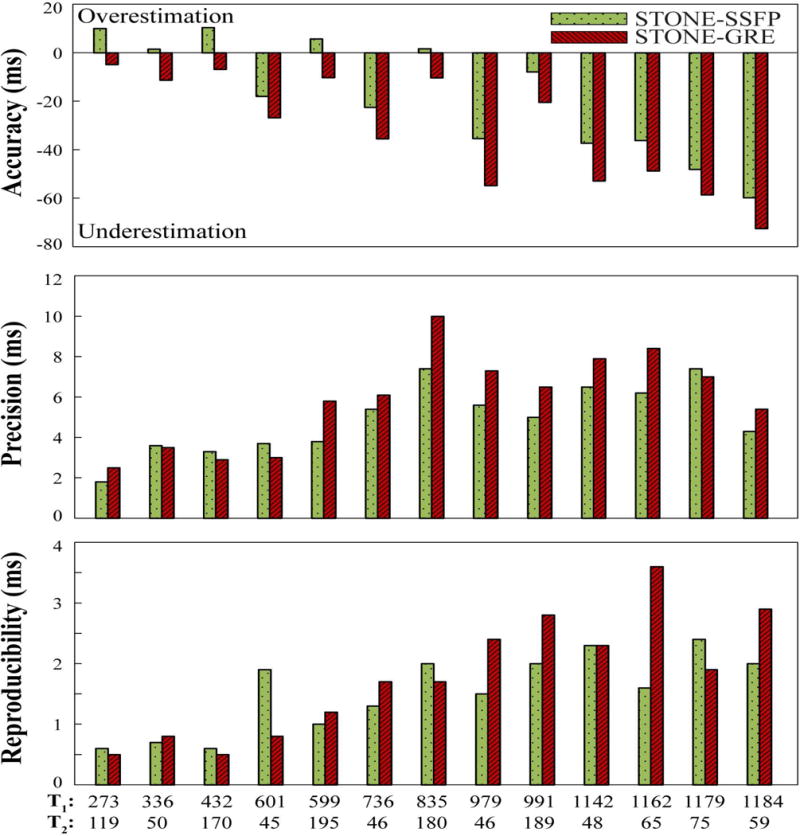
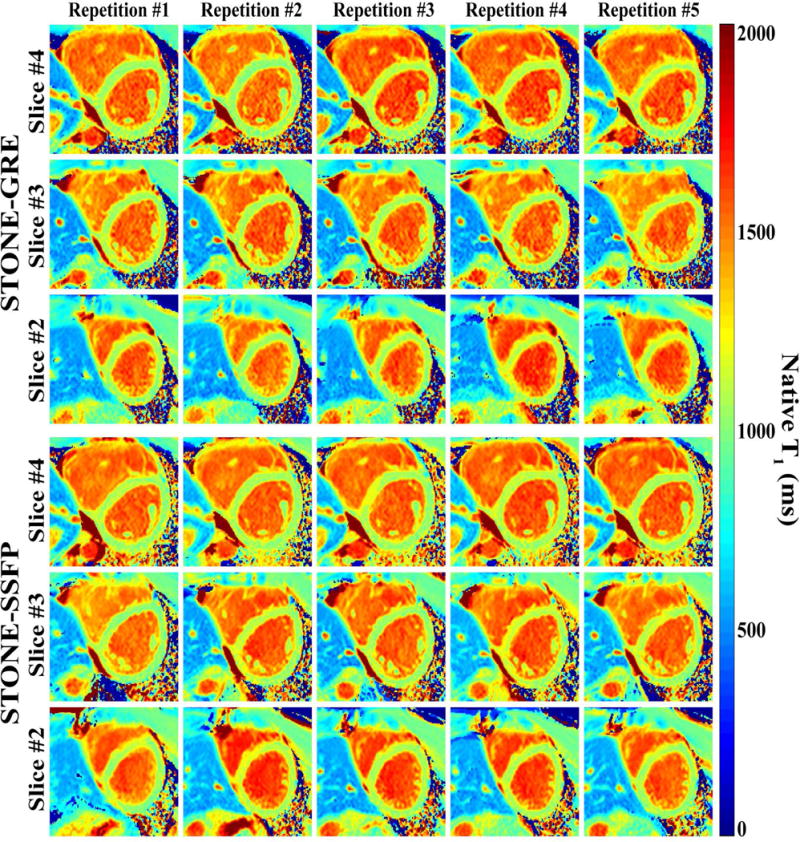
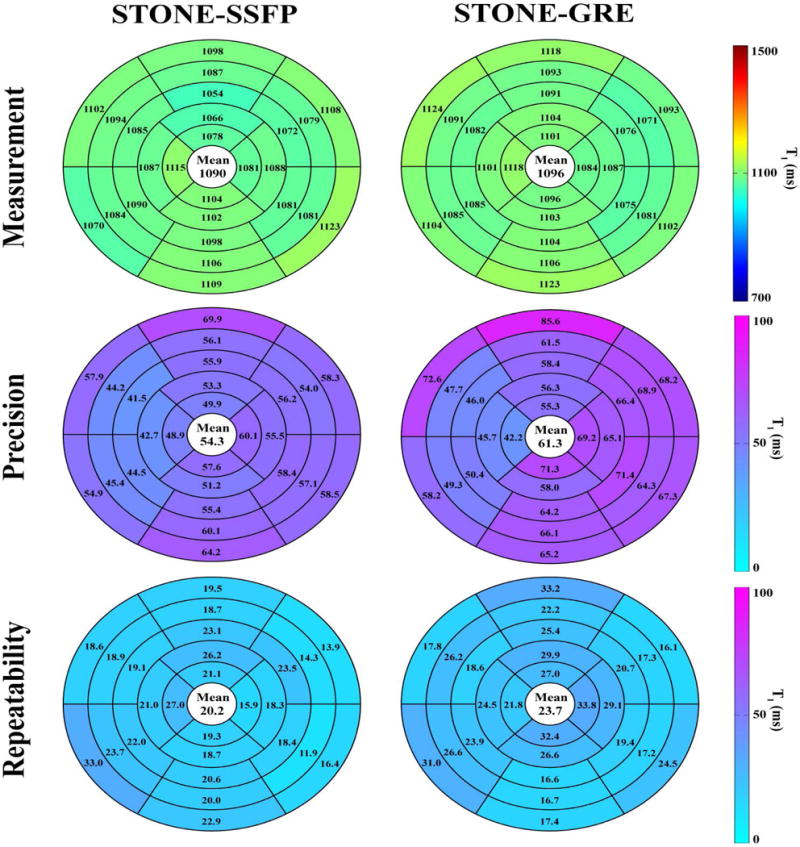
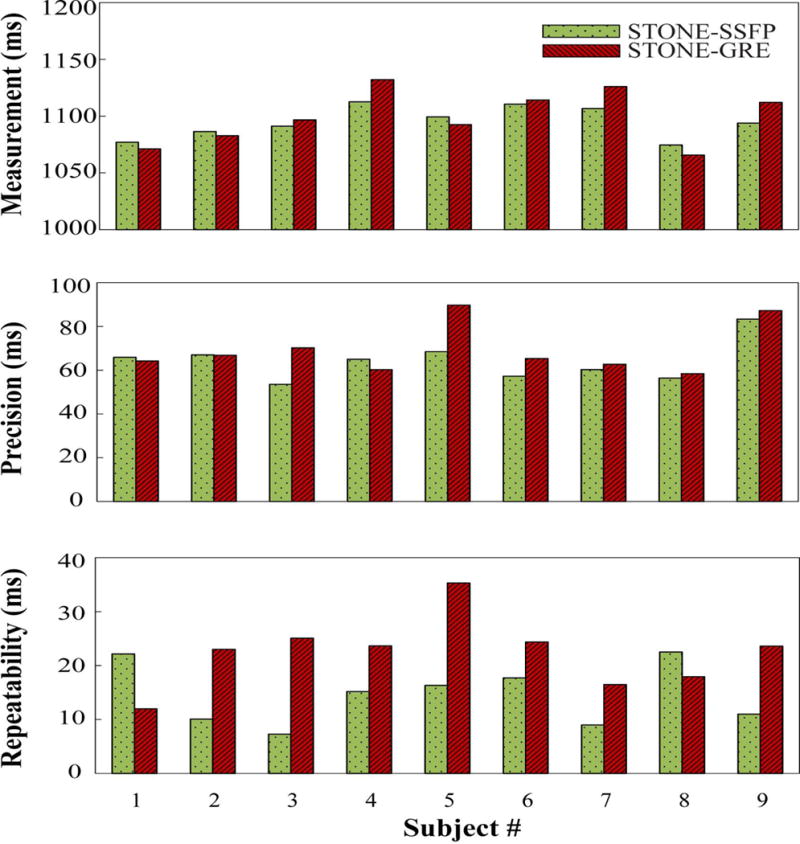
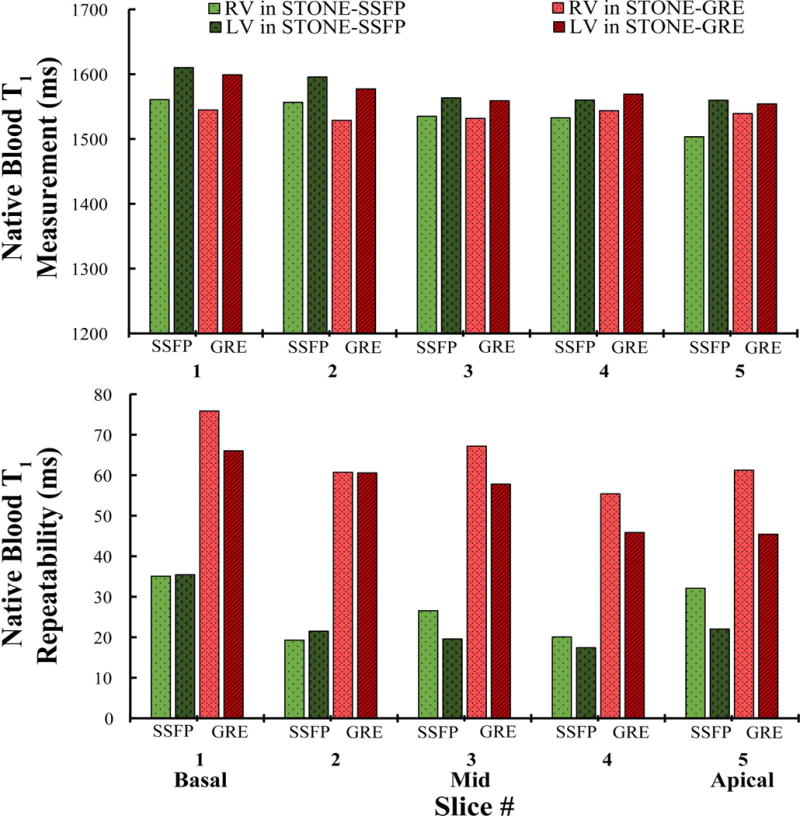
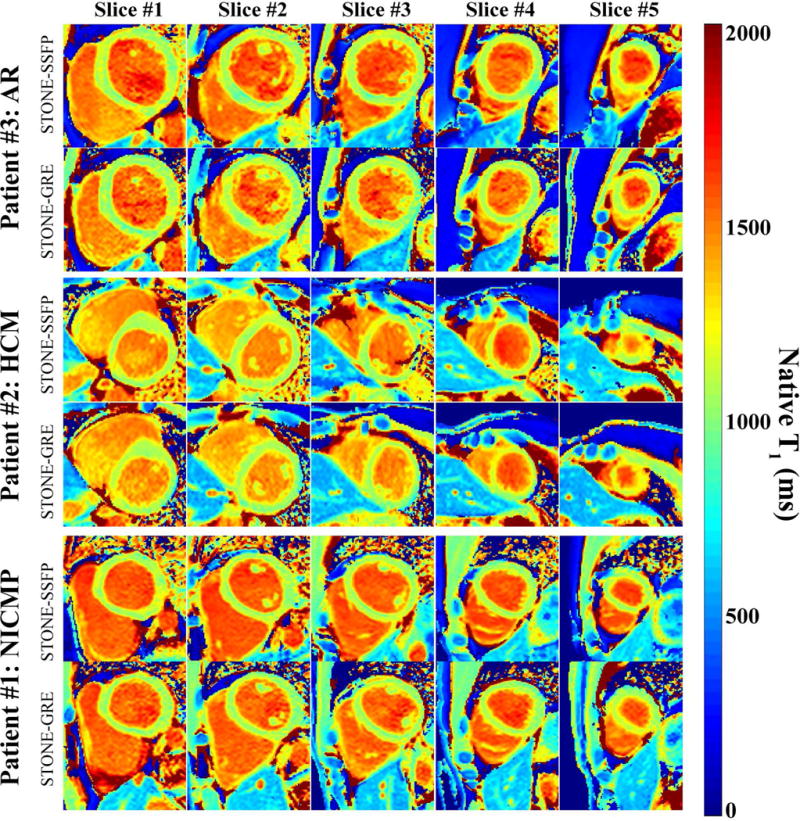
Cardiac T1 mapping allows non-invasive imaging of interstitial diffuse fibrosis. Myocardial T1 is commonly calculated by voxel-wise fitting of the images acquired using balanced steady-state free precession (SSFP) after an inversion pulse. However, SSFP imaging is sensitive to B1 and B0 imperfection, which may result in additional artifacts. A gradient echo (GRE) imaging sequence has been used for myocardial T1 mapping; however, its use has been limited to higher magnetic field to compensate for the lower signal-to-noise ratio (SNR) of GRE versus SSFP imaging. A slice-interleaved T1 mapping (STONE) sequence with SSFP readout (STONE-SSFP) has been recently proposed for native myocardial T1 mapping, which allows longer recovery of magnetization (>8 R-R) after each inversion pulse. In this study, we hypothesize that a longer recovery allows higher SNR and enables native myocardial T1 mapping using STONE with GRE imaging readout (STONE-GRE) at 1.5T. Numerical simulations and phantom and in vivo imaging were performed to compare the performance of STONE-GRE and STONE-SSFP for native myocardial T1 mapping at 1.5T. In numerical simulations, STONE-SSFP shows sensitivity to both T2 and off resonance. Despite the insensitivity of GRE imaging to T2 , STONE-GRE remains sensitive to T2 due to the dependence of the inversion pulse performance on T2 . In the phantom study, STONE-GRE had inferior accuracy and precision and similar repeatability as compared with STONE-SSFP. In in vivo studies, STONE-GRE and STONE-SSFP had similar myocardial native T1 times, precisions, repeatabilities and subjective T1 map qualities. Despite the lower SNR of the GRE imaging readout compared with SSFP, STONE-GRE provides similar native myocardial T1 measurements, precision, repeatability, and subjective image quality when compared with STONE-SSFP at 1.5T.
Keywords: balanced steady-state free precession; cardiovascular MR (CMR) methods; myocardial T1 mapping; relaxometry; slice-interleaved T1 mapping; spoiled gradient echo.
Copyright © 2016 John Wiley & Sons, Ltd.
Figures

References
-
- Messroghli DR, Niendorf T, Schulz-Menger J, Dietz R, Friedrich MG. T1 mapping in patients with acute myocardial infarction. J Cardiovasc Magn Reson. 2003;5(2):353–359. - PubMed
-
- Messroghli DR, Radjenovic A, Kozerke S, Higgins DM, Sivananthan MU, Ridgway JP. Modified Look-Locker inversion recovery (MOLLI) for high-resolution T1 mapping of the heart. Magn Reson Med. 2004;52(1):141–146. - PubMed
-
- Chow K, Flewitt JA, Green JD, Pagano JJ, Friedrich MG, Thompson RB. Saturation recovery single-shot acquisition (SASHA) for myocardial T(1) mapping. Magn Reson Med. 2014;71(6):2082–2095. - PubMed
-
- Weingärtner S, Akcakaya M, Basha T, Kissinger KV, Goddu B, Berg S, Manning WJ, Nezafat R. Combined saturation/inversion recovery sequences for improved evaluation of scar and diffuse fibrosis in patients with arrhythmia or heart rate variability. Magn Reson Med. 2014;71(3):1024–1034. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
