

Systematic identification and management of barriers to vascular surgery patient discharge time of day
- PMID: 27658897
- PMCID: PMC5819890
- DOI: 10.1016/j.jvs.2016.07.109
Systematic identification and management of barriers to vascular surgery patient discharge time of day
Abstract
Objective: Length of stay fails to completely capture the clinical and economic effects of patient progression through the phases of inpatient care, such as admission, room placement, procedures, and discharge. Delayed hospital throughput has been linked to increased time spent in the emergency department and postanesthesia care unit, delayed time to treatment, increased in-hospital mortality, decreased patient satisfaction, and lost hospital revenue. We identified barriers to vascular surgery inpatient care progression and instituted defined measures to positively impact standardized metrics.
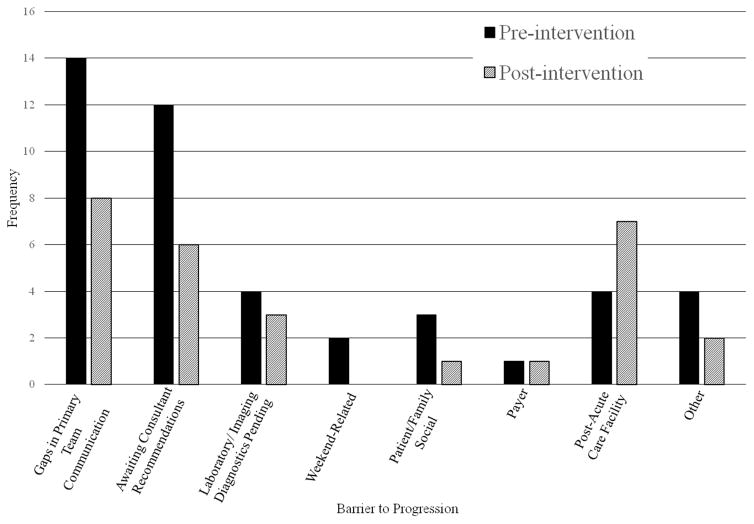
Methods: The study was divided into three periods: preintervention, "wash-in," and postintervention. During the preintervention phase, barriers to patient flow were quantified by an interdisciplinary team. Suboptimal provider communication emerged as the key barrier. An enhanced communication intervention consisting of face-to-face and mobile application-based education on key patient flow metrics, explicit discussion of individual patient barriers to progression at rounds and interdisciplinary huddles, and communication of projected discharge and potential barriers via e-mail was developed with input from all stakeholders. Following a 4-week wash-in implementation phase, data collection was repeated.
Results: The pre- and postintervention patient cohorts accounted for 244.3 and 238.1 inpatient days, respectively. Both groups had similar baseline demographic, clinical characteristics, and procedures performed during hospitalization. The postintervention group was discharged 78 minutes earlier (14:00:32 vs 15:18:37; P = .03) with a trend toward increased discharge by noon (94% vs 88%; P = .09). Readmission rates did not differ (P = .44).
Conclusions: Implementation of a focused, interdisciplinary, frontline provider-driven, enhanced communication program can be feasibly incorporated into existing specialty surgical workflow. The program resulted in improved timeliness of discharge and projected cost savings, without increasing readmission rates.
Copyright © 2016 Society for Vascular Surgery. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.J Vasc Surg. 2017 Jan;65(1):178. doi: 10.1016/j.jvs.2016.07.110. J Vasc Surg. 2017. PMID: 28010857 No abstract available.
References
-
- Pearson SD, Kleefield SF, Soukop JR, Cook EF, Lee TH. Critical pathways intervention to reduce length of hospital stay. Am J Med. 2001;110:175–180. - PubMed
-
- Litvak E, Bisognano M. More patients, less payment: Increasing hospital efficiency in the aftermath of health reform. Health Aff (Millwood) 2011;30:76–80. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
