

Leukoencephalopathy and long-term neurobehavioural, neurocognitive, and brain imaging outcomes in survivors of childhood acute lymphoblastic leukaemia treated with chemotherapy: a longitudinal analysis
- PMID: 27658980
- PMCID: PMC5417340
- DOI: 10.1016/S2352-3026(16)30110-7
Leukoencephalopathy and long-term neurobehavioural, neurocognitive, and brain imaging outcomes in survivors of childhood acute lymphoblastic leukaemia treated with chemotherapy: a longitudinal analysis
Abstract
Background: Leukoencephalopathy is observed in some children undergoing chemotherapy for acute lymphoblastic leukaemia, although its effects on long-term outcomes is unknown. This study examines the associations between acute leukoencephalopathy and neurobehavioural, neurocognitive, and brain white matter imaging outcomes in long-term survivors of childhood acute lymphoblastic leukaemia treated with chemotherapy without cranial radiation.
Methods: In this longitudinal analysis, we used data of children with acute lymphoblastic leukaemia at St Jude Children's Research Hospital (Memphis, TN, USA) who had been treated between June 1, 2000, and Oct 31, 2010. Eligible patients were diagnosed with non-B-cell acute lymphoblastic leukaemia, aged at least 8 years, and survivors with at least 5 years since their initial diagnosis. Brain MRIs obtained during active therapy were systematically coded for leukoencephalopathy using Common Terminology Criteria for Adverse Event version 4. At least 5 years after their diagnosis, survivors completed neurocognitive testing, another brain MRI, and their parents completed neurobehavioural ratings of their child (Behavior Rating Inventory of Executive Function [BRIEF]). Follow-up MRI included diffusion tensor imaging to assess white matter integrity, with indices of fractional anisotropy, axial diffusivity, and radial diffusivity from frontal lobes, parietal lobes, and in the frontostriatal tract. The neuroradiologist, who assessed abnormal MRIs, was masked to both group assignment of survivors and the neurobehavioural and neurocognitive outcomes. The primary outcomes were neurobehavioural function, assessed from completed BRIEF, and neurocognitive performance, measured by direct neurocognitive tests (Delis-Kaplan Executive Function System, Wechsler Intelligence Scale for Children-IV/Wechsler Adult Intelligence Scale-III, Rey-Osterrieth Complex Figure Test, and Lafayette Grooved Pegboard Test). This study had completed enrolment in October, 2014, and is registered as an observational study at ClinicalTrials.gov, number NCT01014195.
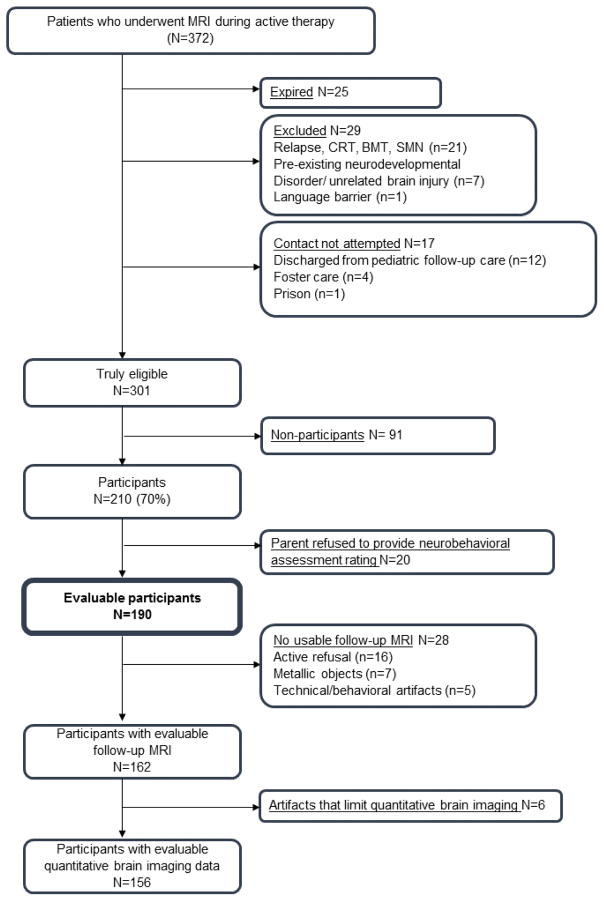
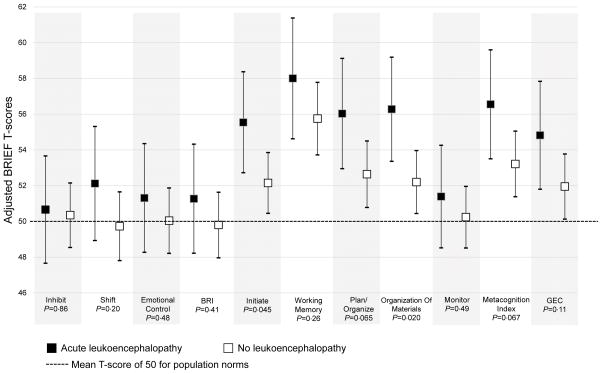
Findings: Between Feb 18, 2010, and Oct 22, 2014, 210 (70%) of 301 eligible survivors participated in our study of whom 190 were evaluable, 162 had an MRI. 56 participants had quantitative brain imaging data and were included in evaluable population analyses. 51 (27%) of the 190 evaluable participants had acute leukoencephalopathy. Compared with population norms, survivors were reported to have more neurobehavioural problems with working memory, organisation, initiation, and planning (p<0·001 for all). Survivors had worse scores than the general population on direct measures of memory span, processing speed, and executive function (p<0·05 for all). Survivors with a history of acute leukoencephalopathy had more neurobehavioural problems than survivors with no history of leukoencephalopathy on organisation (adjusted T-score 56·2 [95% CI 53·3-59·1] vs 52·2 [50·4-53·9], p=0·020) and initiation (55·5 [52·7-58·3] vs 52·1 [50·4-53·8], p=0·045). Survivors with acute leukoencephalopathy also had reduced white matter integrity in the frontostriatal tract at follow-up: lower fractional anisotropy (p=0·069), higher axial diffusivity (p=0·020), and higher radial diffusivity (p=0·0077). A one-unit change in the radial diffusivity index corresponded with a 15·0 increase in raw score points on initiation, 30·3 on planning, and 28·0 on working memory (p<0·05 for all).
Interpretation: Acute leukoencephalopathy during chemotherapy treatment, without cranial radiation, for childhood acute lymphoblastic leukaemia predicted higher risk for long-term neurobehavioural problems and reduced white matter integrity in frontal brain regions. Survivors of childhood acute lymphoblastic leukaemia might benefit from preventive cognitive or behavioural interventions, particularly those who develop acute leukoencephalopathy.
Funding: National Institute of Mental Health, National Cancer Institute, American Lebanese Syrian Associated Charities.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures

References
-
- Pui CH. Toward optimal central nervous system-directed treatment in childhood acute lymphoblastic leukemia. J Clin Oncol. 2003;21(2):179–81. - PubMed
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
