

Fluid-Attenuated Inversion Recovery Vascular Hyperintensity Topography, Novel Imaging Marker for Revascularization in Middle Cerebral Artery Occlusion
- PMID: 27659851
- PMCID: PMC5079823
- DOI: 10.1161/STROKEAHA.116.013953
Fluid-Attenuated Inversion Recovery Vascular Hyperintensity Topography, Novel Imaging Marker for Revascularization in Middle Cerebral Artery Occlusion
Abstract
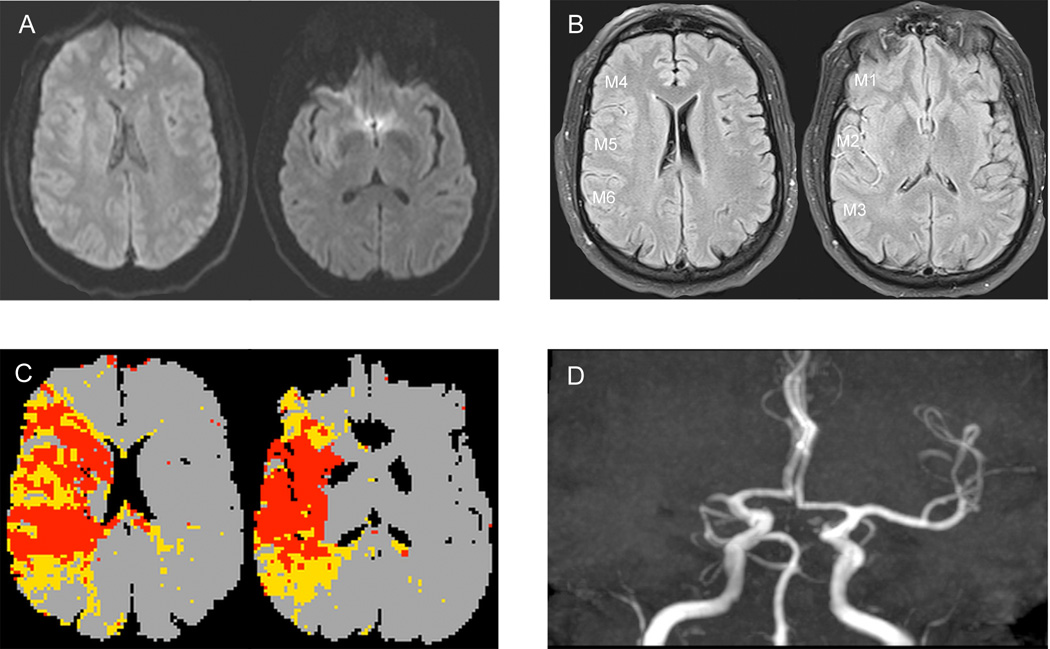
Background and purpose: In acute arterial occlusion, fluid-attenuated inversion recovery vascular hyperintensity (FVH) has been linked to slow flow in leptomeningeal collaterals and cerebral hypoperfusion, but the impact on clinical outcome is still controversial. In this study, we aimed to investigate the association between FVH topography or FVH-Alberta Stroke Program Early CT Score (ASPECTS) pattern and outcome in acute M1-middle cerebral artery occlusion patients with endovascular treatment.
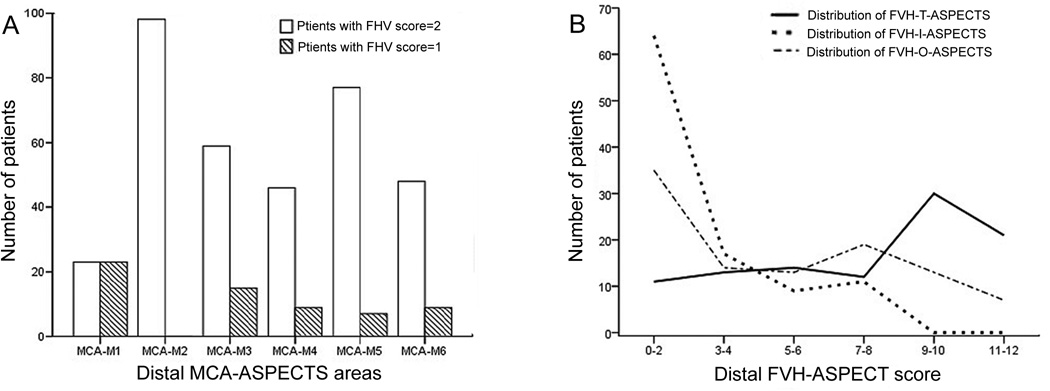
Methods: We included acute M1-middle cerebral artery occlusion patients treated with endovascular therapy (ET). All patients had diffusion-weighted imaging (DWI) and fluid-attenuated inversion recovery before ET. Distal FVH-ASPECTS was evaluated according to distal middle cerebral artery-ASPECT area (M1-M6) and acute DWI lesion was also reviewed. The presence of FVH inside and outside DWI-positive lesions was separately analyzed. Clinical outcome after ET was analyzed with respect to different distal FVH-ASPECTS topography.
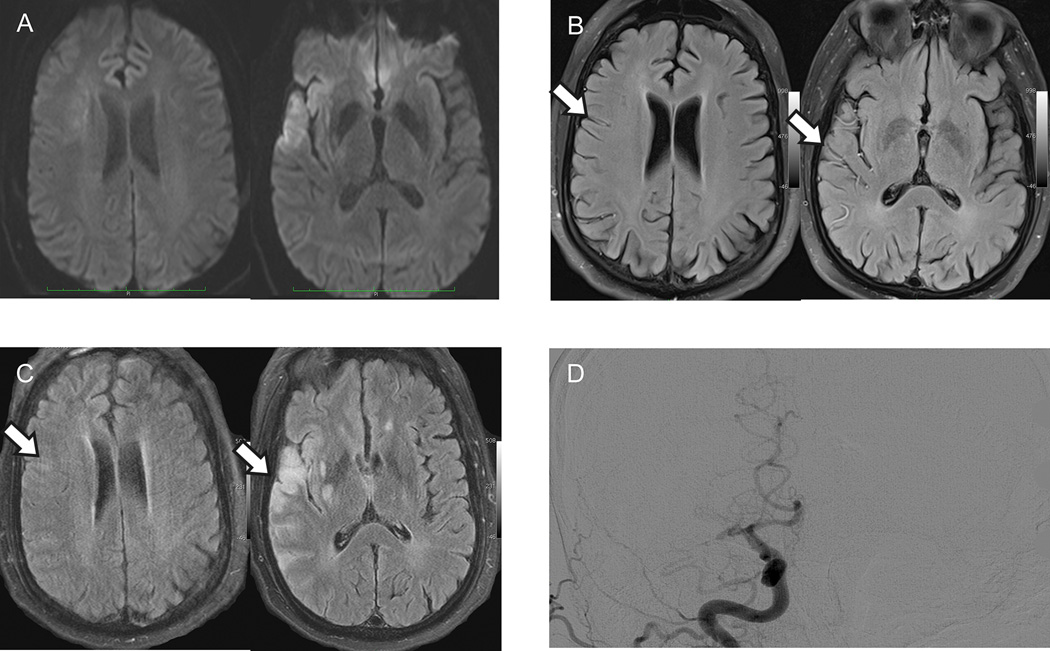
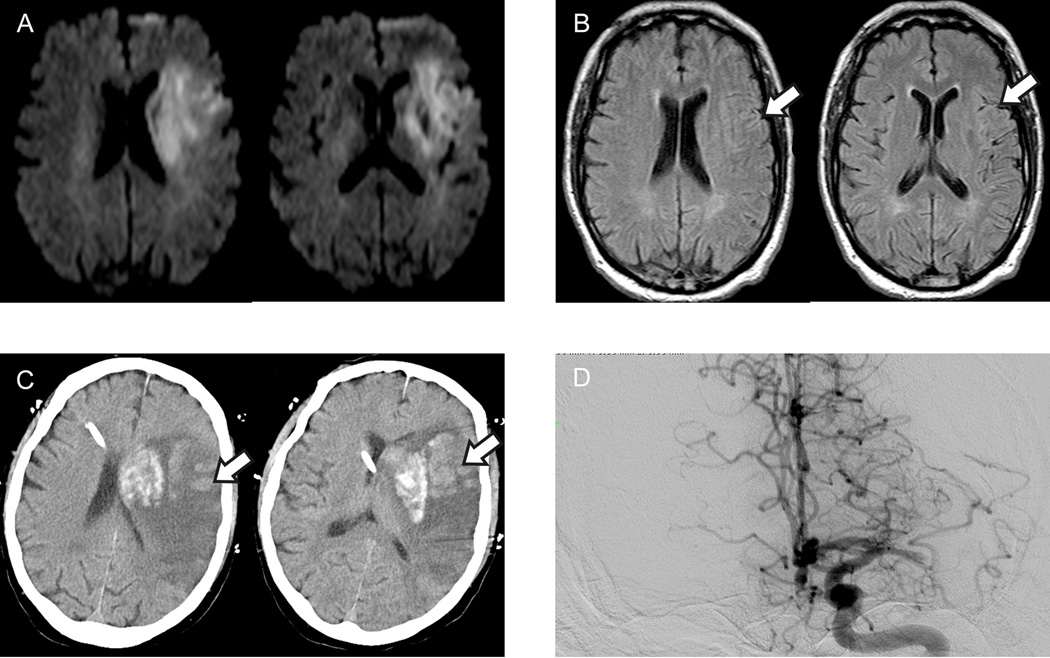
Results: Among 101 patients who met inclusion criteria for the study, mean age was 66.2±17.8 years and median National Institutes of Health Stroke Scale was 17.0 (interquartile range, 12.0-21.0). FVH-ASPECTS measured outside of the DWI lesion was significantly higher in patients with good outcome (modified Rankin Scale [mRS] score of 0-2; 8.0 versus 4.0, P<0.001). Logistic regression demonstrated that FVH-ASPECTS outside of the DWI lesion was independently associated with clinical outcome of these patients (odds ratio, 1.3; 95% confidence interval, 1.06-1.68; P=0.013). FVH-ASPECTS inside the DWI lesion was associated with hemorrhagic transformation (odds ratio, 1.3; 95% confidence interval, 1.04-1.51; P=0.019).
Conclusions: Higher FVH-ASPECTS measured outside the DWI lesion is associated with good clinical outcomes in patients undergoing ET. FVH-ASPECTS measured inside the DWI lesion was predictive of hemorrhagic transformation. The FVH pattern, not number, can serve as an imaging selection marker for ET in acute middle cerebral artery occlusion.
Keywords: hypertension; magnetic resonance imaging; middle cerebral artery occlusion; stroke; thrombectomy.
© 2016 American Heart Association, Inc.
Figures
Similar articles
-
Fluid-attenuated inversion recovery vascular hyperintensity-diffusion-weighted imaging mismatch and functional outcome after endovascular reperfusion therapy for acute ischemic stroke.Interv Neuroradiol. 2024 Apr;30(2):189-194. doi: 10.1177/15910199221113900. Epub 2022 Jul 29. Interv Neuroradiol. 2024. PMID: 35903941 Free PMC article.
-
Benefit from revascularization after thrombectomy according to FLAIR vascular hyperintensities-DWI mismatch.Eur Radiol. 2019 Oct;29(10):5567-5576. doi: 10.1007/s00330-019-06094-y. Epub 2019 Mar 22. Eur Radiol. 2019. PMID: 30903341
-
Fluid-Attenuated Inversion Recovery Vascular Hyperintensities-Diffusion-Weighted Imaging Mismatch Identifies Acute Stroke Patients Most Likely to Benefit From Recanalization.Stroke. 2016 Feb;47(2):424-7. doi: 10.1161/STROKEAHA.115.010999. Epub 2016 Jan 5. Stroke. 2016. PMID: 26732567
-
Indications for Mechanical Thrombectomy-Too Wide or Too Narrow?World Neurosurg. 2019 Jul;127:492-499. doi: 10.1016/j.wneu.2019.04.116. Epub 2019 Apr 19. World Neurosurg. 2019. PMID: 31009772 Review.
-
Mechanical recanalization for acute bilateral cerebral artery occlusion - literature overview with a case.Radiol Oncol. 2020 Mar 26;54(2):144-148. doi: 10.2478/raon-2020-0017. Radiol Oncol. 2020. PMID: 32229680 Free PMC article.
Cited by
-
Clot Burden Score and Collateral Status and Their Impact on Functional Outcome in Acute Ischemic Stroke.AJNR Am J Neuroradiol. 2021 Jan;42(1):42-48. doi: 10.3174/ajnr.A6865. Epub 2020 Nov 12. AJNR Am J Neuroradiol. 2021. PMID: 33184069 Free PMC article.
-
New vessels formation in young strokes with isolated steno-occlusive MCA.Brain Behav. 2018 Oct;8(10):e01088. doi: 10.1002/brb3.1088. Epub 2018 Sep 15. Brain Behav. 2018. PMID: 30260098 Free PMC article.
-
FLAIR Vascular Hyperintensities as a Surrogate of Collaterals in Acute Stroke: DWI Matters.AJNR Am J Neuroradiol. 2023 Jan;44(1):26-32. doi: 10.3174/ajnr.A7733. Epub 2022 Dec 15. AJNR Am J Neuroradiol. 2023. PMID: 36521962 Free PMC article.
-
Prognostic value of post-treatment fluid-attenuated inversion recovery vascular hyperintensity in ischemic stroke after endovascular thrombectomy.Eur Radiol. 2022 Dec;32(12):8067-8076. doi: 10.1007/s00330-022-08886-1. Epub 2022 Jun 3. Eur Radiol. 2022. PMID: 35665844
-
FLAIR Vascular Hyperintensities as Imaging Biomarker in Pediatric Acute Ischemic Stroke.Stroke. 2025 Jun;56(6):1505-1515. doi: 10.1161/STROKEAHA.124.048717. Epub 2025 Mar 28. Stroke. 2025. PMID: 40151929
References
-
- Turc G, Apoil M, Naggara O, Calvet D, Lamy C, Tataru AM, et al. Magnetic resonance imaging-dragon score: 3-month outcome prediction after intravenous thrombolysis for anterior circulation stroke. Stroke; a journal of cerebral circulation. 2013;44:1323–1328. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
