

Incidences and variations of hospital acquired venous thromboembolism in Australian hospitals: a population-based study
- PMID: 27659903
- PMCID: PMC5034410
- DOI: 10.1186/s12913-016-1766-y
Incidences and variations of hospital acquired venous thromboembolism in Australian hospitals: a population-based study
Abstract
Background: Data on hospital-acquired venous thromboembolism (HA-VTE) incidence, case fatality rate and variation amongst patient groups and health providers is lacking. We aim to explore HA-VTE incidences, associated mortality, trends and variations across all acute hospitals in New South Wales (NSW)-Australia.
Methods: A population-based study using all admitted patients (aged 18-90 with a length of stay of at least two days and not transferred to another acute care facility) in 104 NSW acute public and private hospitals during 2002-2009. Poisson mixed models were used to derive adjusted rate ratios (IRR) in presence of patient and hospital characteristics.
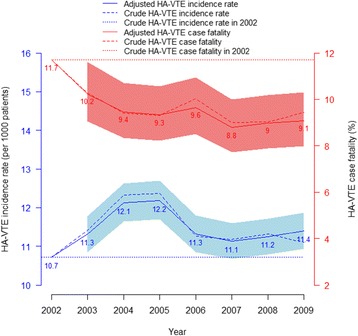
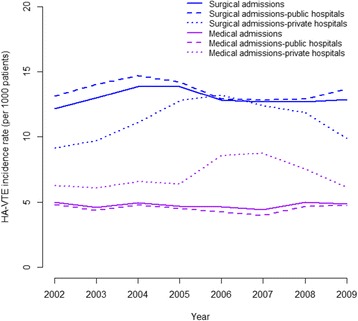
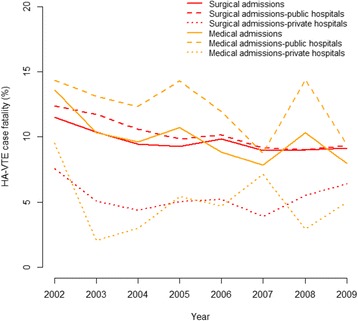
Results: Amongst, 3,331,677 patients, the incidence of HA-VTE was 11.45 per 1000 patients and one in ten who developed HA-VTE died in hospital. HA-VTE incidence, initially rose, but subsequently declined, whereas case fatality rate consistently declined by 22 % over the study period. Surgical patients were 128 % (IRR = 2.28, 95 % CI: 2.19-2.38) more likely to develop HA-VTE, but had similar case fatality rates compared to medical patients. Private hospitals, in comparison to public hospitals had a higher incidence of HA-VTE (IRR = 1.76; 95 % CI: 1.42-2.18) for medical patients. However, they had a similar incidence (IRR = 0.91; 95 % CI: 0.75-1.11), but a lower mortality (IRR = 0.59; 95 % CI: 0.47-0.75) amongst surgical patients. Smaller public hospitals had a lower HA-VTE incidence rate compared to larger hospitals (IRR < 0.68) but a higher case fatality rate (IRR > 1.71). Hospitals with a lower reported HA-VTE incidence tended to have a higher HA-VTE case fatality rate.
Conclusion: Despite the decline in HA-VTE incidence and case fatality, there were large variations in incidents between medical and surgical patients, public and private hospitals, and different hospital groups. The causes of such differences warrant further investigation and may provide potential for targeted interventions and quality improvement initiatives.
Keywords: Hospital acquired complication; Patient safety; Quality improvement; Venous thromboembolism.
Figures
References
-
- National Health and Medical Research Council . Preventing venous thromboembolism in hospitalised patients: summary of NHMRC activity 2003–2010. Melbourne: NHMRC; 2011.
-
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism a statement for healthcare professionals from the Council on Thrombosis (in Consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996;93(12):2212–45. doi: 10.1161/01.CIR.93.12.2212. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
