

Pharmacokinetic Evaluation of the Tau PET Radiotracer 18F-T807 (18F-AV-1451) in Human Subjects
- PMID: 27660144
- PMCID: PMC5334185
- DOI: 10.2967/jnumed.115.170910
Pharmacokinetic Evaluation of the Tau PET Radiotracer 18F-T807 (18F-AV-1451) in Human Subjects
Abstract
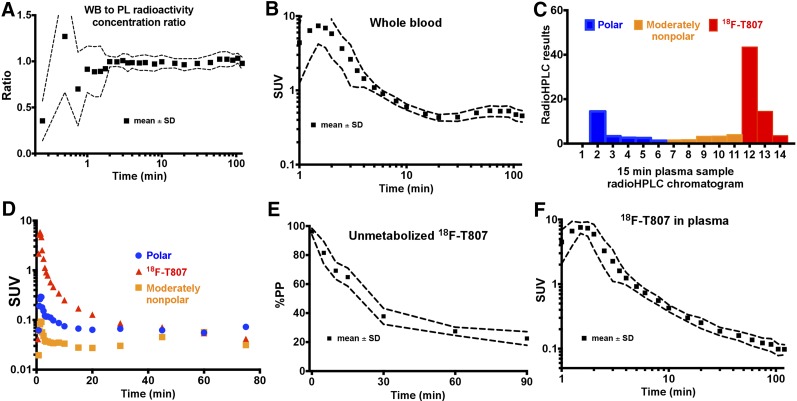
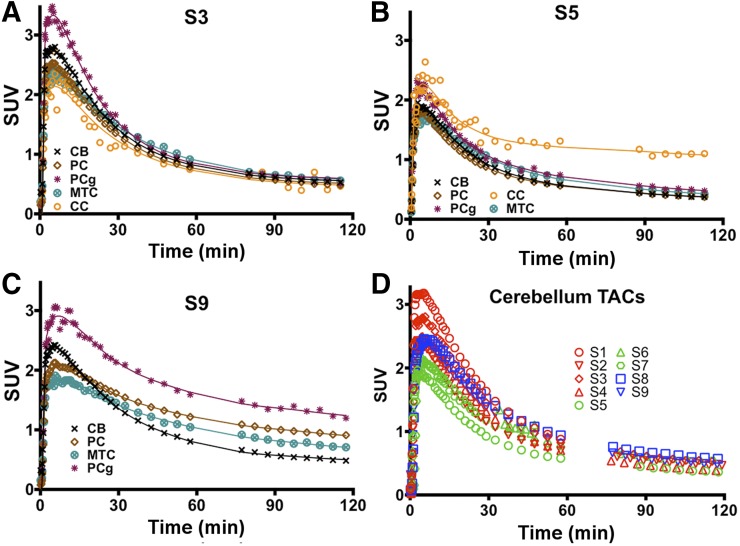
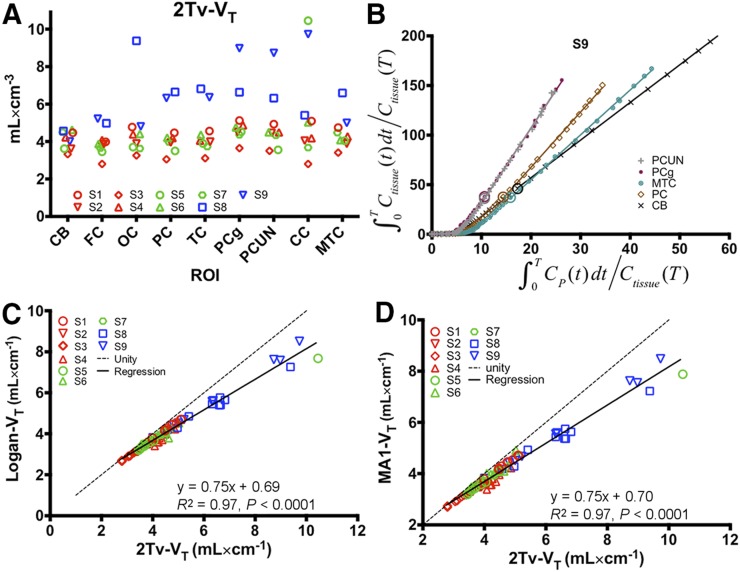
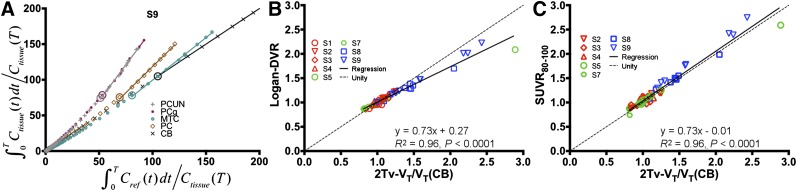
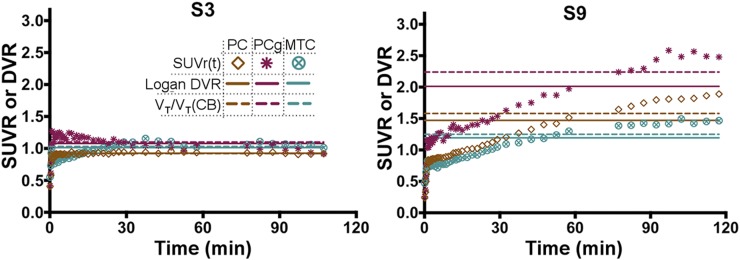
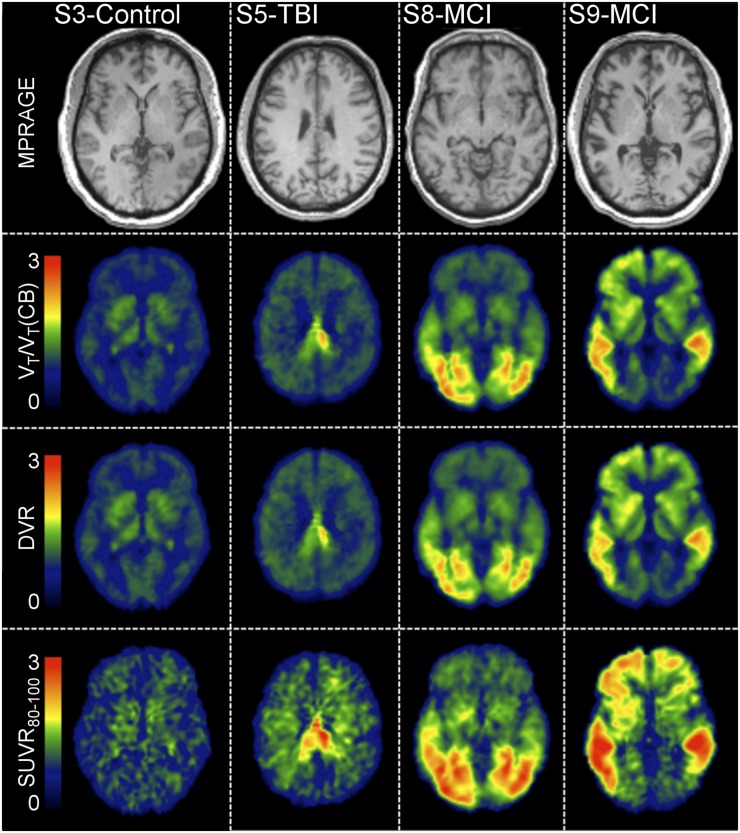
18F-T807 is a PET radiotracer developed for imaging tau protein aggregates, which are implicated in neurologic disorders including Alzheimer disease and traumatic brain injury (TBI). The current study characterizes 18F-T807 pharmacokinetics in human subjects using dynamic PET imaging and metabolite-corrected arterial input functions. Methods: Nine subjects (4 controls, 3 with a history of TBI, 2 with mild cognitive impairment due to suspected Alzheimer disease) underwent dynamic PET imaging for up to 120 min after bolus injection of 18F-T807 with arterial blood sampling. Total volume of distribution (VT) was estimated using compartmental modeling (1- and 2-tissue configurations) and graphical analysis techniques (Logan and multilinear analysis 1 [MA1] regression methods). Reference region-based methods of quantification were explored including Logan distribution volume ratio (DVR) and static SUV ratio (SUVR) using the cerebellum as a reference tissue. Results: The percentage of unmetabolized 18F-T807 in plasma followed a single exponential with a half-life of 17.0 ± 4.2 min. Metabolite-corrected plasma radioactivity concentration fit a biexponential (half-lives, 18.1 ± 5.8 and 2.4 ± 0.5 min). 18F-T807 in gray matter peaked quickly (SUV > 2 at ∼5 min). Compartmental modeling resulted in good fits, and the 2-tissue model with estimated blood volume correction (2Tv) performed best, particularly in regions with elevated binding. VT was greater in mild cognitive impairment subjects than controls in the occipital, parietal, and temporal cortices as well as the posterior cingulate gyrus, precuneus, and mesial temporal cortex. High focal uptake was found in the posterior corpus callosum of a TBI subject. Plots from Logan and MA1 graphical methods became linear by 30 min, yielding regional estimates of VT in excellent agreement with compartmental analysis and providing high-quality parametric maps when applied in voxelwise fashion. Reference region-based approaches including Logan DVR (t* = 55 min) and SUVR (80- to 100-min interval) were highly correlated with DVR estimated using 2Tv (R2 = 0.97, P < 0.0001). Conclusion:18F-T807 showed rapid clearance from plasma and properties suitable for tau quantification with PET. Furthermore, simplified approaches using DVR (t* = 55 min) and static SUVR (80-100 min) with cerebellar reference tissue were found to correlate highly with compartmental modeling outcomes.
Keywords: 18F-T807; PET; kinetic modeling; pharmacokinetics; tau.
© 2017 by the Society of Nuclear Medicine and Molecular Imaging.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources