

Predictors of Cognitive Decline in Older Adult Type 2 Diabetes from the Veterans Affairs Diabetes Trial
- PMID: 27660621
- PMCID: PMC5015004
- DOI: 10.3389/fendo.2016.00123
Predictors of Cognitive Decline in Older Adult Type 2 Diabetes from the Veterans Affairs Diabetes Trial
Abstract
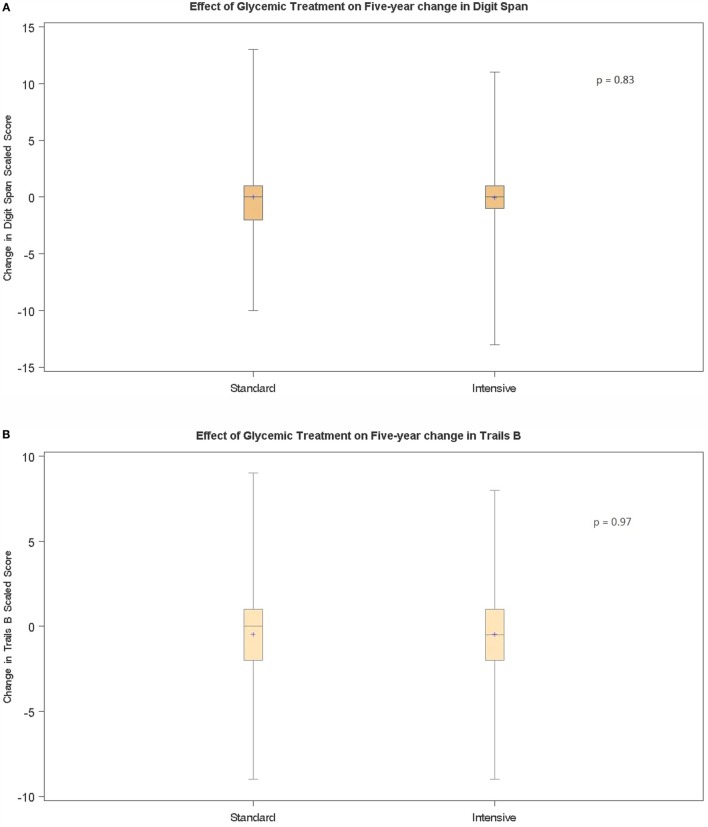
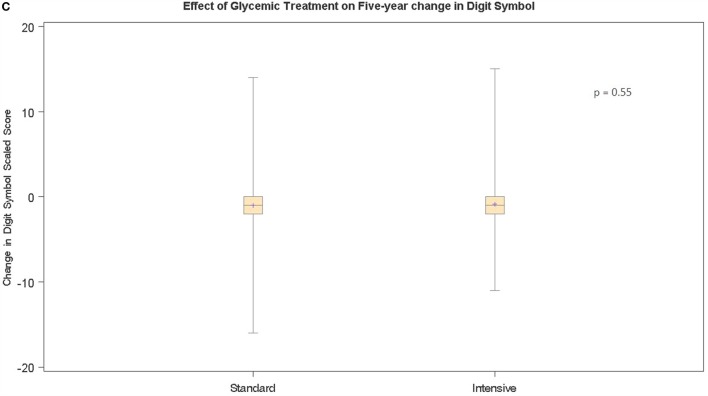
Aims: Cognitive decline disproportionately affects older adult type 2 diabetes. We tested whether randomized intensive (INT) glucose-lowering reduces the rate(s) of cognitive decline in adults with advanced type 2 diabetes (mean: age, 60 years; diabetes duration, 11 years) from the Veterans Affairs Diabetes Trial.
Methods: A battery of neuropsychological tests [digit span, digit symbol substitution (DSym), and Trails-making Test-Part B (TMT-B)] was administered at baseline in ~1700 participants and repeated at year 5. Thirty-seven risk factors were evaluated as predictors of cognitive decline in multivariable regression analyses.
Results: The mean age-adjusted DSym or TMT-B declined significantly in all study participants (P < 0.001). Randomized INT glucose-lowering did not significantly alter the rate of cognitive decline. The final model of risk factors associated with 5-year decline in age-adjusted TMT-B included as significant predictors: longer baseline diabetes duration (beta = -0.028; P = 0.0057), lower baseline diastolic blood pressure (BP; beta = 0.028; P = 0.002), and baseline calcium channel blocker medication use (beta = -0.639; P < 0.001). Higher baseline pulse pressure was significantly associated with decline in age-adjusted TMT-B suggesting a role for both higher systolic and lower diastolic BPs. Baseline thiazide diuretic use (beta = -0.549; P = 0.015) was an additional significant predictor of 5-year decline in age-adjusted digit symbol score. Post-baseline systolic BP-lowering was significantly associated (P < 0.001) with decline in TMT-B performance. There was a significant inverse association between post-baseline plasma triglyceride-lowering (P = 0.045) and decline in digit symbol substitution task performance.
Conclusion: A 5-year period of randomized INT glucose-lowering did not significantly reduce the rate of cognitive decline in older-aged adults with type 2 diabetes. Systolic and diastolic BPs as well as plasma triglycerides appeared as modifiable risk factors of the rate of cognitive decline in older adult type 2 diabetes.
Keywords: blood pressure; cognitive decline; diabetes duration; risk factors; type 2 diabetes mellitus.
Figures
References
-
- Launer LJ, Miller ME, Williamson JD, Lazar RM, Gerstein HC, Murray AM, et al. Effects of intensive glucose lowering on brain structure and function in people with type 2 diabetes (ACCORD MIND): a randomised open-label substudy. Lancet Neurol (2011) 10(11):969–77.10.1016/S1474-4422(11)70188-0 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical