

Autograft versus allograft in anterior cruciate ligament reconstruction: A meta-analysis with trial sequential analysis
- PMID: 27661048
- PMCID: PMC5044918
- DOI: 10.1097/MD.0000000000004936
Autograft versus allograft in anterior cruciate ligament reconstruction: A meta-analysis with trial sequential analysis
Abstract
Background: Anterior cruciate ligament (ACL) reconstruction is considered as the standard surgical procedure for the treatment of ACL tear. However, there is a crucial controversy in terms of whether to use autograft or allograft in ACL reconstruction. The purpose of this meta-analysis is to compare autograft with allograft for patients undergoing ACL reconstruction.
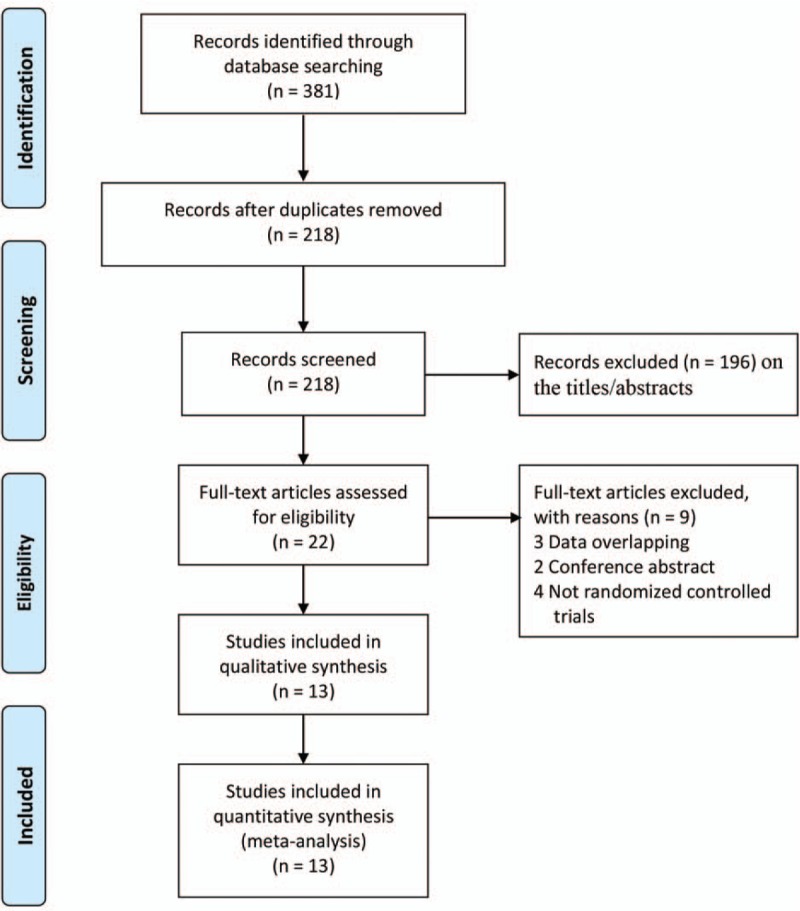
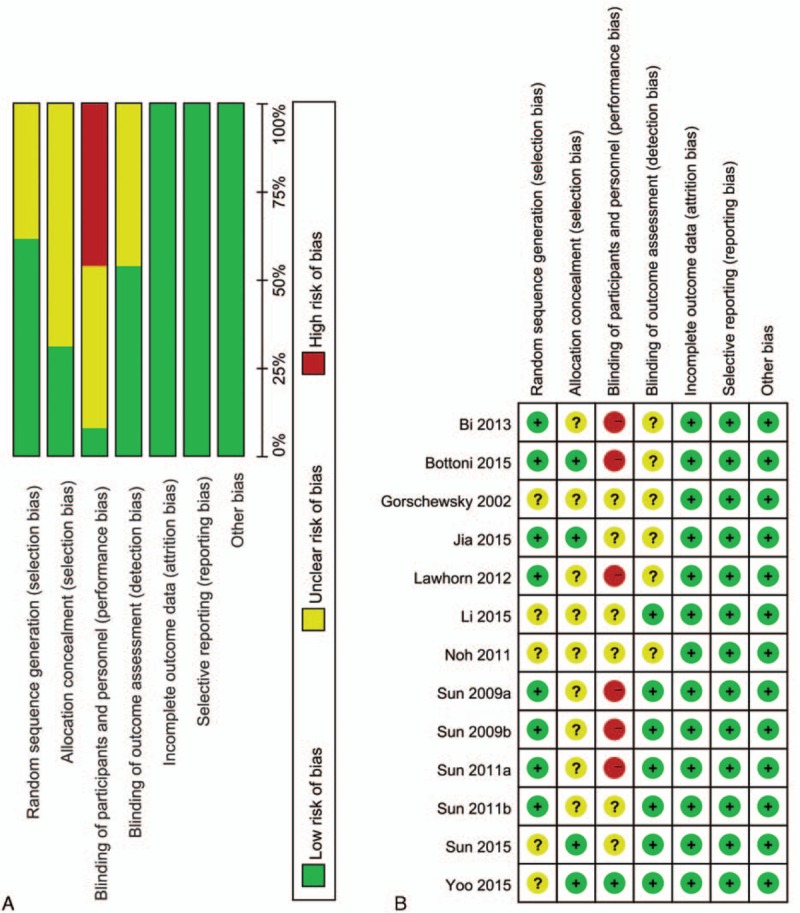
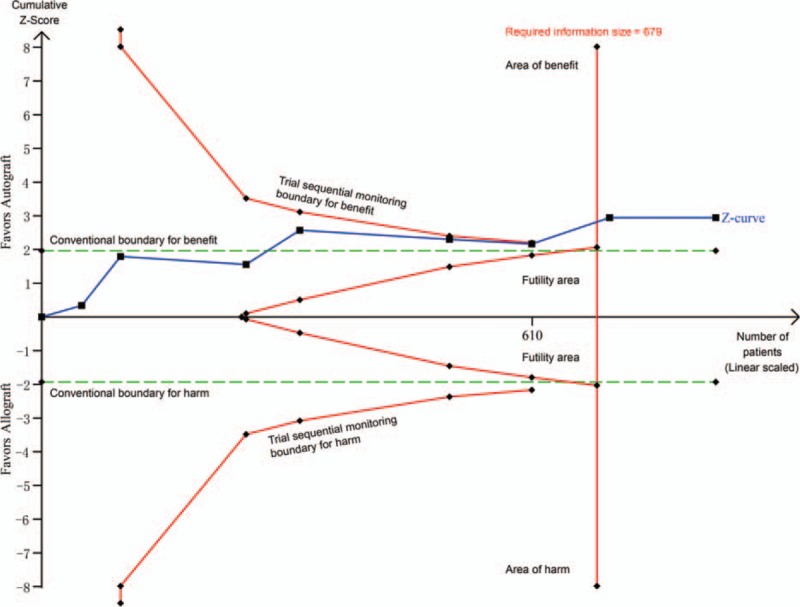
Methods: PubMed, EMBASE, and the Cochrane Library were searched for randomized controlled trials that compared autograft with allograft in ACL reconstruction up to January 31, 2016. The relative risk or mean difference with 95% confidence interval was calculated using either a fixed- or random-effects model. The risk of bias for individual studies according to the Cochrane Handbook. The trial sequential analysis was used to test the robustness of our findings and get more conservative estimates.
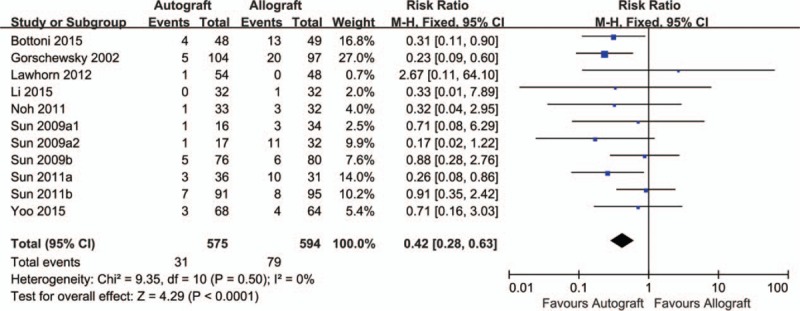
Results: Thirteen trials were included, involving 1636 participants. The results of this meta-analysis indicated that autograft brought about lower clinical failure, better overall International Knee Documentation Committee (IKDC) level, better pivot-shift test, better Lachman test, greater Tegner score, and better instrumented laxity test (P < 0.05) than allograft. Autograft was not statistically different from allograft in Lysholm score, subjective IKDC score, and Daniel 1-leg hop test (P > 0.05). Subgroup analyses demonstrated that autograft was superior to irradiated allograft for patients undergoing ACL reconstruction in clinical failure, Lysholm score, pivot-shift test, Lachman test, Tegner score, instrumented laxity test, and subjective IKDC score (P < 0.05). Moreover, there were no significant differences between autograft and nonirradiated allograft.
Conclusions: Autograft is superior to irradiated allograft for patients undergoing ACL reconstruction concerning knee function and laxity, but there are no significant differences between autograft and nonirradiated allograft. However, our results should be interpreted with caution, because the blinding methods were not well used.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Moses B, Orchard J, Orchard J. Systematic review: annual incidence of ACL injury and surgery in various populations. Res Sports Med 2012; 20:157–179. - PubMed
-
- Cimino F, Volk BS, Setter D. Anterior cruciate ligament injury: diagnosis, management, and prevention. Am Family Physic 2010; 82:917–922. - PubMed
-
- Engebretsen L, Benum P, Fasting O, et al. A prospective, randomized study of three surgical techniques for treatment of acute ruptures of the anterior cruciate ligament. Am J Sports Med 1990; 18:585–590. - PubMed
-
- Daniel DM, Stone ML, Dobson BE, et al. Fate of the ACL-injured patient. A prospective outcome study. Am J Sports Med 1994; 22:632–644. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
