

Feasibility of MR-Based Body Composition Analysis in Large Scale Population Studies
- PMID: 27662190
- PMCID: PMC5035023
- DOI: 10.1371/journal.pone.0163332
Feasibility of MR-Based Body Composition Analysis in Large Scale Population Studies
Abstract
Introduction: Quantitative and accurate measurements of fat and muscle in the body are important for prevention and diagnosis of diseases related to obesity and muscle degeneration. Manually segmenting muscle and fat compartments in MR body-images is laborious and time-consuming, hindering implementation in large cohorts. In the present study, the feasibility and success-rate of a Dixon-based MR scan followed by an intensity-normalised, non-rigid, multi-atlas based segmentation was investigated in a cohort of 3,000 subjects.
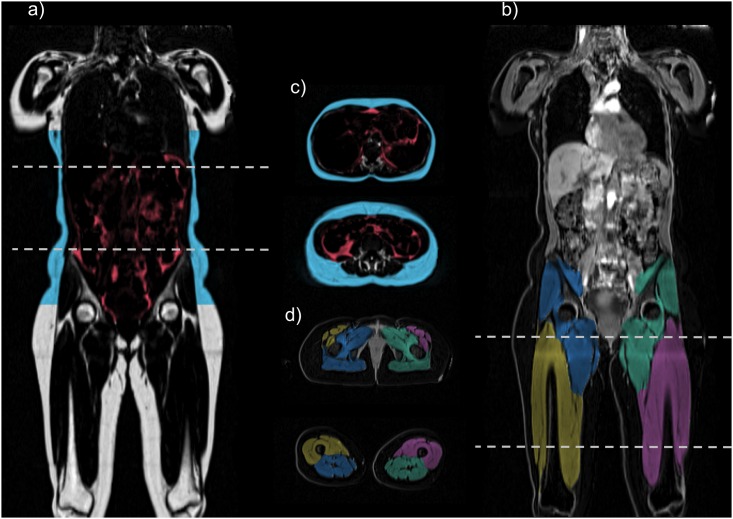
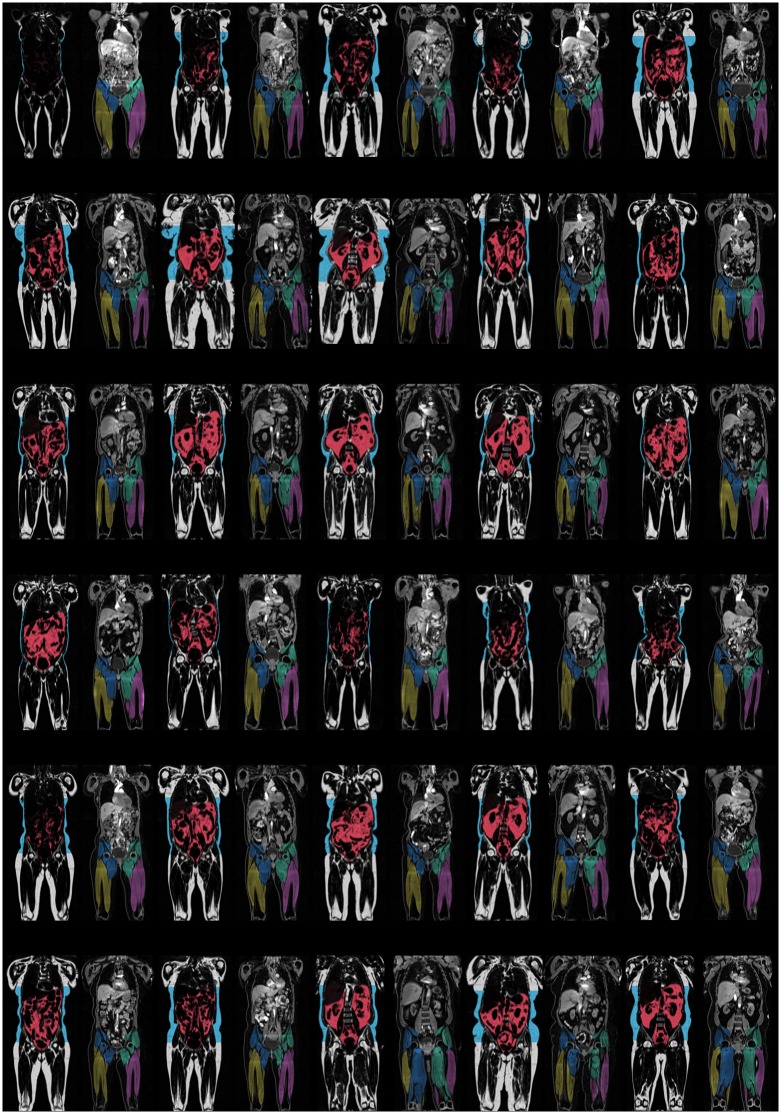
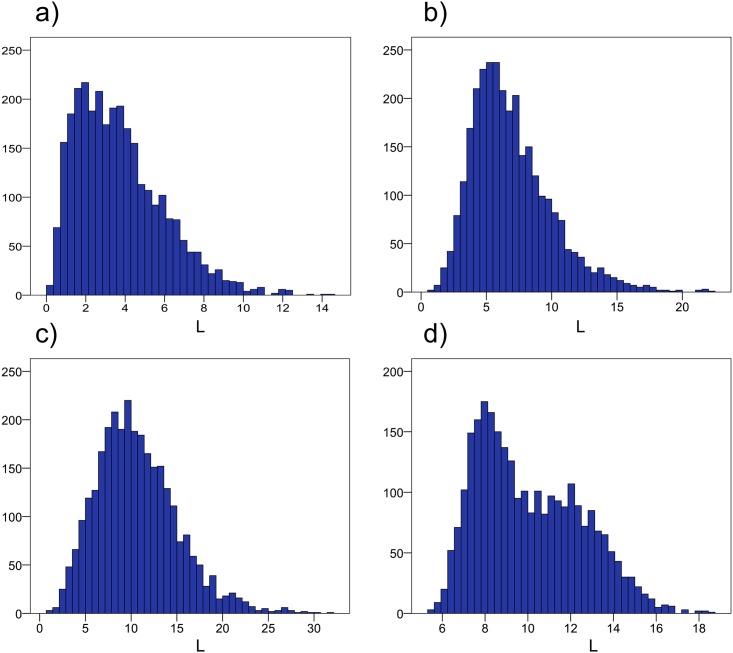
Materials and methods: 3,000 participants in the in-depth phenotyping arm of the UK Biobank imaging study underwent a comprehensive MR examination. All subjects were scanned using a 1.5 T MR-scanner with the dual-echo Dixon Vibe protocol, covering neck to knees. Subjects were scanned with six slabs in supine position, without localizer. Automated body composition analysis was performed using the AMRA Profiler™ system, to segment and quantify visceral adipose tissue (VAT), abdominal subcutaneous adipose tissue (ASAT) and thigh muscles. Technical quality assurance was performed and a standard set of acceptance/rejection criteria was established. Descriptive statistics were calculated for all volume measurements and quality assurance metrics.
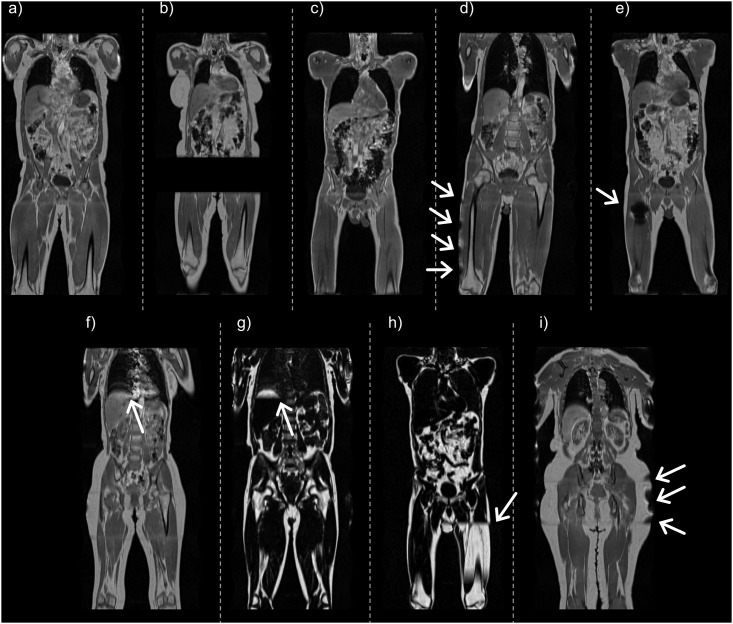
Results: Of the 3,000 subjects, 2,995 (99.83%) were analysable for body fat, 2,828 (94.27%) were analysable when body fat and one thigh was included, and 2,775 (92.50%) were fully analysable for body fat and both thigh muscles. Reasons for not being able to analyse datasets were mainly due to missing slabs in the acquisition, or patient positioned so that large parts of the volume was outside of the field-of-view.
Discussion and conclusions: In conclusion, this study showed that the rapid UK Biobank MR-protocol was well tolerated by most subjects and sufficiently robust to achieve very high success-rate for body composition analysis. This research has been conducted using the UK Biobank Resource.
Conflict of interest statement
JW, ODL, TR, and MB are stock holders in Advanced MR Analytics (AMRA). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- WHO. Global status report on noncommunicable diseases 2014. Geneva, Switzerland: WHO Press; 2014. 298 p.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
