

Implantation of the Medtronic Harmony Transcatheter Pulmonary Valve Improves Right Ventricular Size and Function in an Ovine Model of Postoperative Chronic Pulmonary Insufficiency
- PMID: 27662847
- PMCID: PMC6563325
- DOI: 10.1161/CIRCINTERVENTIONS.116.003920
Implantation of the Medtronic Harmony Transcatheter Pulmonary Valve Improves Right Ventricular Size and Function in an Ovine Model of Postoperative Chronic Pulmonary Insufficiency
Abstract
Background: Pulmonary insufficiency is the nexus of late morbidity and mortality after transannular patch repair of tetralogy of Fallot. This study aimed to establish the feasibility of implantation of the novel Medtronic Harmony transcatheter pulmonary valve (hTPV) and to assess its effect on pulmonary insufficiency and ventricular function in an ovine model of chronic postoperative pulmonary insufficiency.
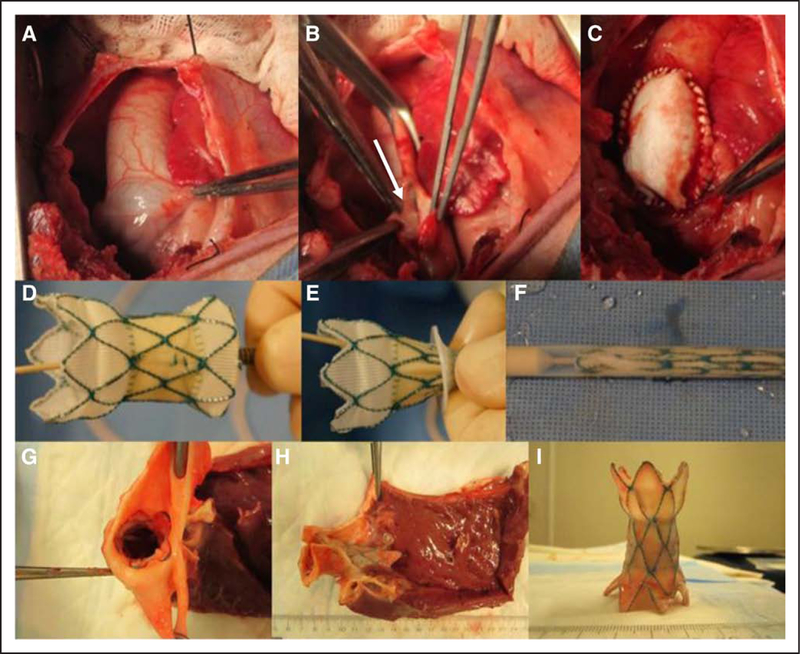
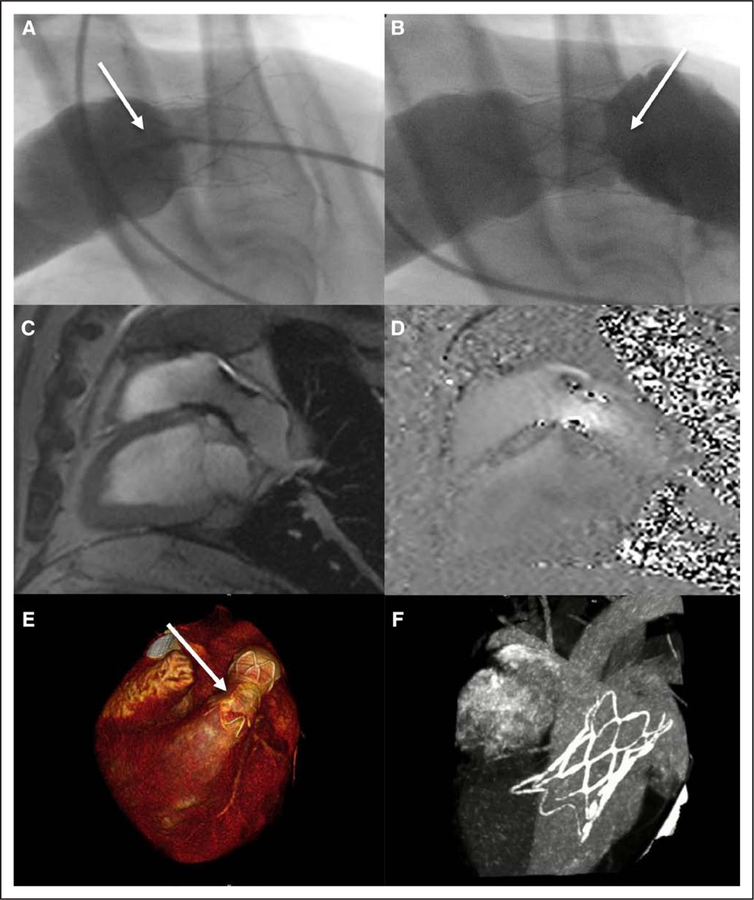
Methods and results: Thirteen sheep underwent baseline cardiac magnetic resonance imaging, surgical pulmonary valvectomy, and transannular patch repair. One month after transannular patch repair, the hTPV was implanted, followed by serial magnetic resonance imaging and computed tomography imaging at 1, 5, and 8 month(s). hTPV implantation was successful in 11 animals (85%). There were 2 procedural deaths related to ventricular fibrillation. Seven animals survived the entire follow-up protocol, 5 with functioning hTPV devices. Two animals had occlusion of hTPV with aneurysm of main pulmonary artery. A strong decline in pulmonary regurgitant fraction was observed after hTPV implantation (40.5% versus 8.3%; P=0.011). Right ventricular end diastolic volume increased by 49.4% after transannular patch repair (62.3-93.1 mL/m2; P=0.028) but was reversed to baseline values after hTPV implantation (to 65.1 mL/m2 at 8 months, P=0.045). Both right ventricular ejection fraction and left ventricular ejection fraction were preserved after hTPV implantation.
Conclusions: hTPV implantation is feasible, significantly reduces pulmonary regurgitant fraction, facilitates right ventricular volume improvements, and preserves biventricular function in an ovine model of chronic pulmonary insufficiency. This percutaneous strategy could potentially offer an alternative for standard surgical pulmonary valve replacement in dilated right ventricular outflow tracts, permitting lower risk, nonsurgical pulmonary valve replacement in previously prohibitive anatomies.
Keywords: cardiac catheterization; computed tomography; heart valve prosthesis implantation; magnetic resonance imaging; pulmonary valve regurgitation; tetralogy of Fallot.
© 2016 American Heart Association, Inc.
Conflict of interest statement
Disclosures
Dr Gillespie serves as a consultant to Medtronic, the manufacturer of the hTPV device. Dr Litt receives research funding from Siemens Healthcare for unrelated projects. The other authors report no conflicts.
Figures






References
-
- Al Habib HF, Jacobs JP, Mavroudis C, Tchervenkov CI, O’Brien SM, Mohammadi S, Jacobs ML. Contemporary patterns of management of tetralogy of Fallot: data from the Society of Thoracic Surgeons Database. Ann Thorac Surg 2010;90:813–819, discussion 819. doi: 10.1016/j.athoracsur.2010.03.110. - DOI - PubMed
-
- Ferraz Cavalcanti PE, Sá MP, Santos CA, Esmeraldo IM, de Escobar RR, de Menezes AM, de Azevedo OM Jr, de Vasconcelos Silva FP, Lins RF, Lima Rde C. Pulmonary valve replacement after operative repair of tetralogy of Fallot: meta-analysis and meta-regression of 3,118 patients from 48 studies. J Am Coll Cardiol 2013;62:2227–2243. doi: 10.1016/j.jacc.2013.04.107. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
