

Clinical Predictors of Hospital Mortality Differ Between Direct and Indirect ARDS
- PMID: 27663180
- PMCID: PMC5472517
- DOI: 10.1016/j.chest.2016.09.004
Clinical Predictors of Hospital Mortality Differ Between Direct and Indirect ARDS
Abstract
Background: Direct (pulmonary) and indirect (extrapulmonary) ARDS are distinct syndromes with important pathophysiologic differences. The goal of this study was to determine whether clinical characteristics and predictors of mortality differ between direct or indirect ARDS.
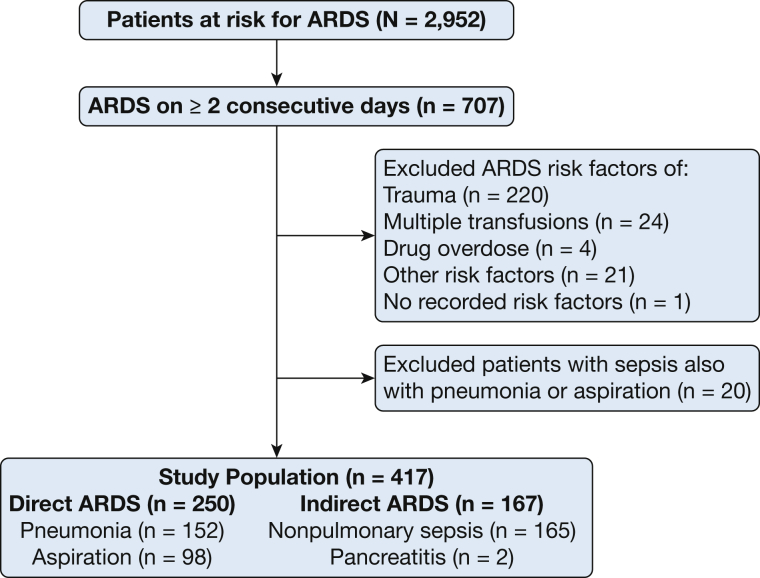
Methods: This retrospective observational cohort study included 417 patients with ARDS. Each patient was classified as having direct (pneumonia or aspiration, n = 250) or indirect (nonpulmonary sepsis or pancreatitis, n = 167) ARDS.
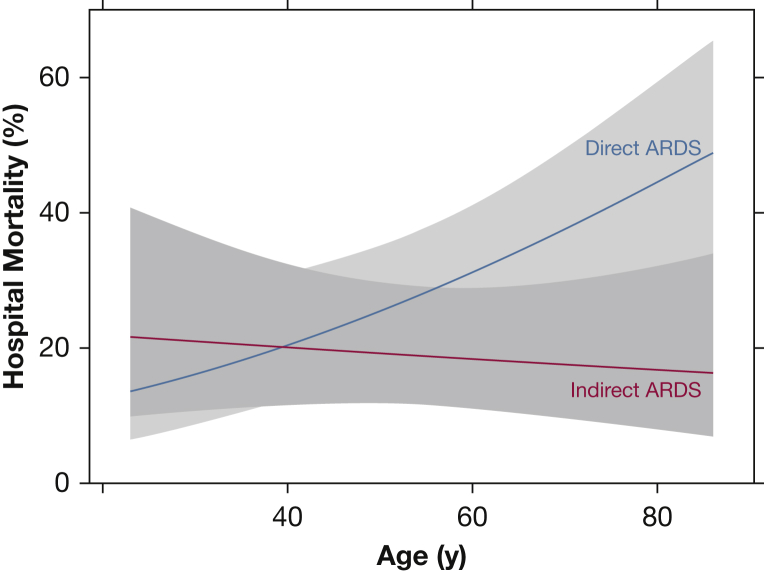
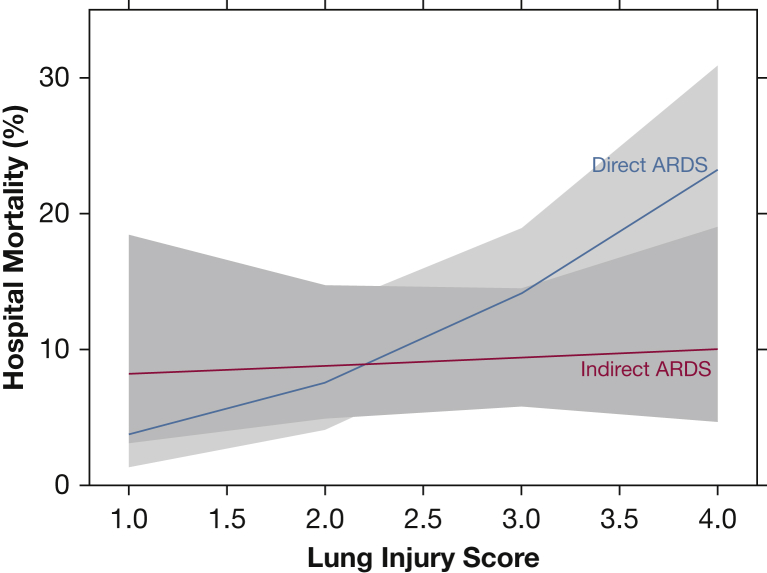
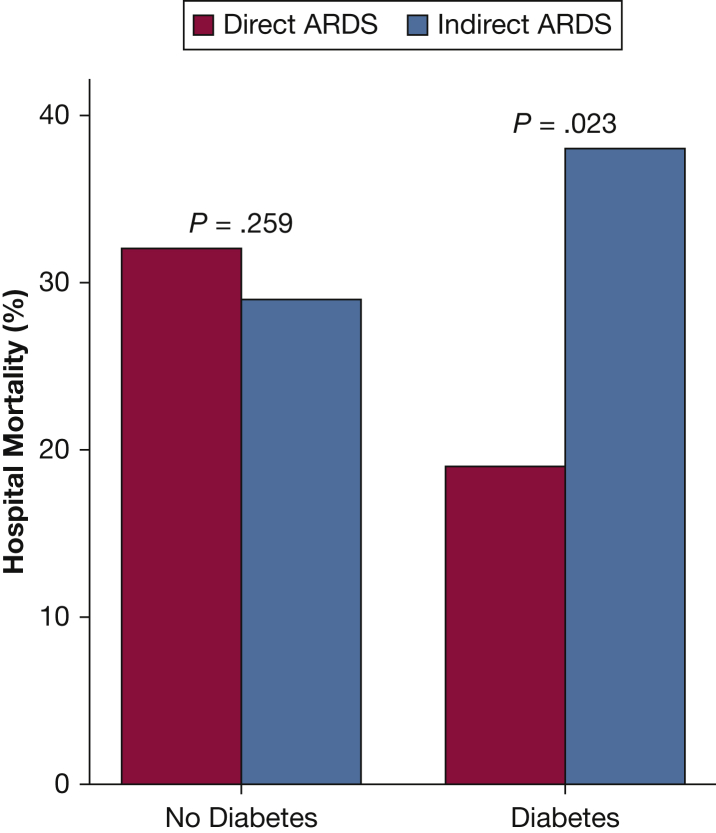
Results: Patients with direct ARDS had higher lung injury scores (3.0 vs 2.8; P < .001), lower Simplified Acute Physiology Score II scores (51 vs 62; P < .001), lower Acute Physiology and Chronic Health Evaluation II scores (27 vs 30; P < .001), and fewer nonpulmonary organ failures (1 vs 2; P < .001) compared with patients with indirect ARDS. Hospital mortality was similar (28% vs 31%). In patients with direct ARDS, age (OR, 1.29 per 10 years; P = .01; test for interaction, P = .03), lung injury scores (OR, 2.29 per point; P = .001; test for interaction, P = .058), and number of nonpulmonary organ failures (OR, 1.67; P = .01) were independent risk factors for increased hospital mortality. Preexisting diabetes mellitus was an independent risk factor for reduced hospital mortality (OR, 0.47; P = .04; test for interaction, P = .02). In indirect ARDS, only the number of organ failures was an independent predictor of mortality (OR, 2.08; P < .001).
Conclusions: Despite lower severity of illness and fewer organ failures, patients with direct ARDS had mortality rates similar to patients with indirect ARDS. Factors previously associated with mortality during ARDS were only associated with mortality in direct ARDS. These findings suggest that direct and indirect ARDS have distinct features that may differentially affect risk prediction and clinical outcomes.
Keywords: ARDS; diabetes; direct lung injury; indirect lung injury; mortality.
Copyright © 2016 American College of Chest Physicians. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
In ARDS, Heterogeneity = Opportunity.Chest. 2017 Apr;151(4):731-732. doi: 10.1016/j.chest.2016.11.016. Chest. 2017. PMID: 28390623 No abstract available.
Similar articles
-
Outcomes of acute respiratory distress syndrome (ARDS) in elderly patients.J Trauma. 2007 Aug;63(2):344-50. doi: 10.1097/TA.0b013e3180eea5a1. J Trauma. 2007. PMID: 17693834
-
Distinct molecular phenotypes of direct vs indirect ARDS in single-center and multicenter studies.Chest. 2015 Jun;147(6):1539-1548. doi: 10.1378/chest.14-2454. Chest. 2015. PMID: 26033126 Free PMC article. Clinical Trial.
-
Nonpulmonary risk factors of acute respiratory distress syndrome in patients with septic bacteraemia.Korean J Intern Med. 2019 Jan;34(1):116-124. doi: 10.3904/kjim.2017.204. Epub 2018 Jun 14. Korean J Intern Med. 2019. PMID: 29898577 Free PMC article.
-
Etiology and outcomes of pulmonary and extrapulmonary acute lung injury/ARDS in a respiratory ICU in North India.Chest. 2006 Sep;130(3):724-9. doi: 10.1378/chest.130.3.724. Chest. 2006. PMID: 16963669
-
Time to change diagnostic criteria of ARDS: towards the disease entity-based subgrouping.Pulm Pharmacol Ther. 2005;18(2):115-9. doi: 10.1016/j.pupt.2004.11.001. Pulm Pharmacol Ther. 2005. PMID: 15712404 Review.
Cited by
-
Artificial intelligence for mechanical ventilation: systematic review of design, reporting standards, and bias.Br J Anaesth. 2022 Feb;128(2):343-351. doi: 10.1016/j.bja.2021.09.025. Epub 2021 Nov 9. Br J Anaesth. 2022. PMID: 34772497 Free PMC article.
-
The Association Between Etiologies and Mortality in Acute Respiratory Distress Syndrome: A Multicenter Observational Cohort Study.Front Med (Lausanne). 2021 Oct 18;8:739596. doi: 10.3389/fmed.2021.739596. eCollection 2021. Front Med (Lausanne). 2021. PMID: 34733862 Free PMC article.
-
Plasma microRNAs levels are different between pulmonary and extrapulmonary ARDS patients: a clinical observational study.Ann Intensive Care. 2018 Feb 13;8(1):23. doi: 10.1186/s13613-018-0370-1. Ann Intensive Care. 2018. PMID: 29442256 Free PMC article.
-
Dual Roles of Hypoxia-Inducible Factor 1 in Acute Lung Injury: Tissue-Specific Mechanisms and Therapeutic Modulation.Cells. 2025 Jul 16;14(14):1089. doi: 10.3390/cells14141089. Cells. 2025. PMID: 40710342 Free PMC article. Review.
-
Acute Respiratory Distress Syndrome: Pathophysiological Insights, Subphenotypes, and Clinical Implications-A Comprehensive Review.J Clin Med. 2025 Jul 22;14(15):5184. doi: 10.3390/jcm14155184. J Clin Med. 2025. PMID: 40806804 Free PMC article. Review.
References
-
- Rubenfeld G.D., Caldwell E., Peabody E. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353(16):1685–1693. - PubMed
-
- Goss C.H., Brower R.G., Hudson L.D. Incidence of acute lung injury in the United States. Crit Care Med. 2003;31(6):1607–1611. - PubMed
-
- Caser E.B., Zandonade E., Pereira E. Impact of distinct definitions of acute lung injury on its incidence and outcomes in Brazilian ICUs: prospective evaluation of 7,133 patients. Crit Care Med. 2014;42(3):574–582. - PubMed
-
- Ranieri V.M., Rubenfeld G.D., Thompson B.T. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012;307(23):2526–2533. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
