

A noninvasive swallowing measurement system using a combination of respiratory flow, swallowing sound, and laryngeal motion
- PMID: 27665103
- PMCID: PMC5440489
- DOI: 10.1007/s11517-016-1561-2
A noninvasive swallowing measurement system using a combination of respiratory flow, swallowing sound, and laryngeal motion
Abstract
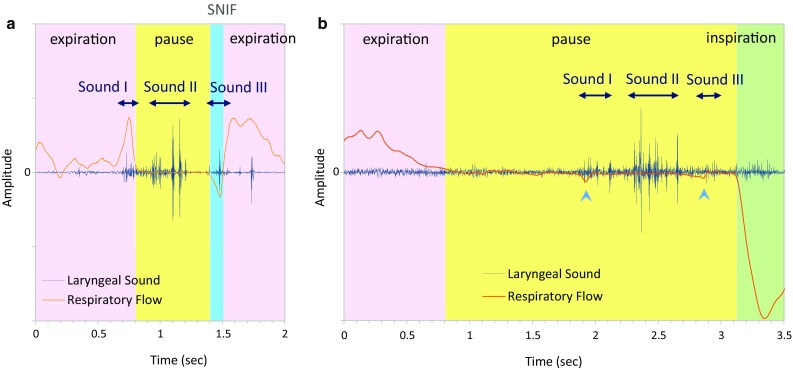
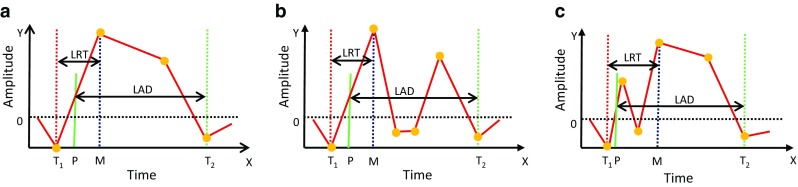
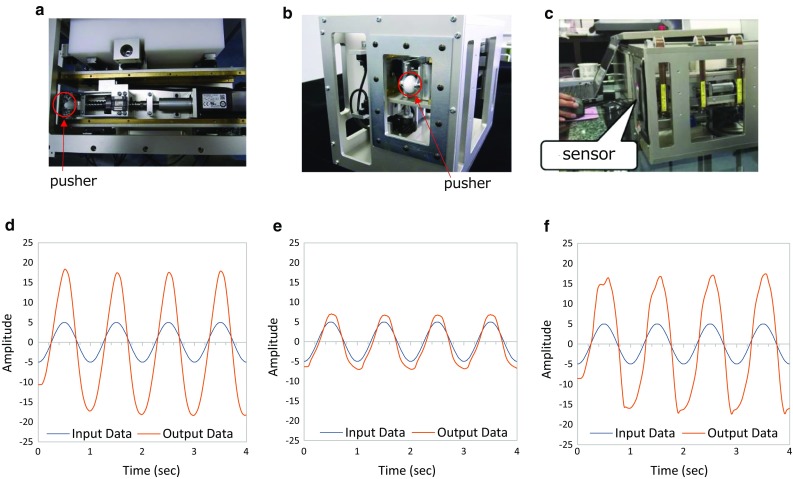
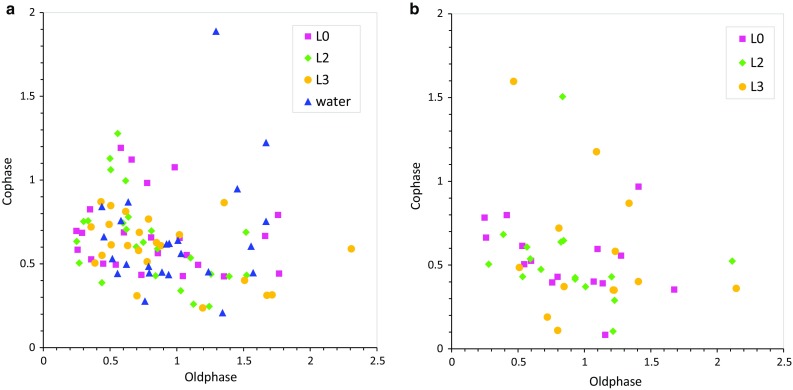
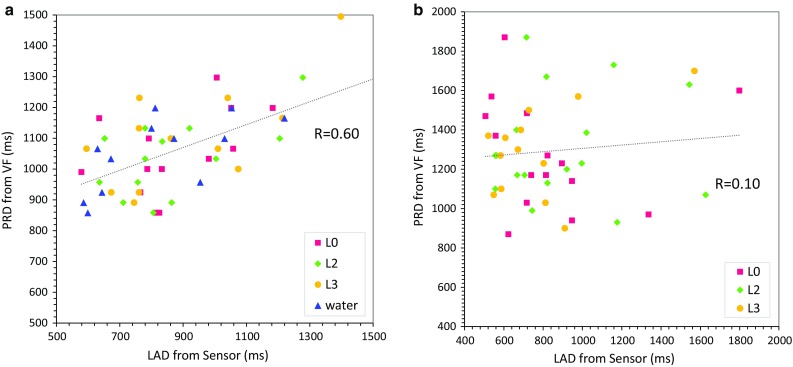
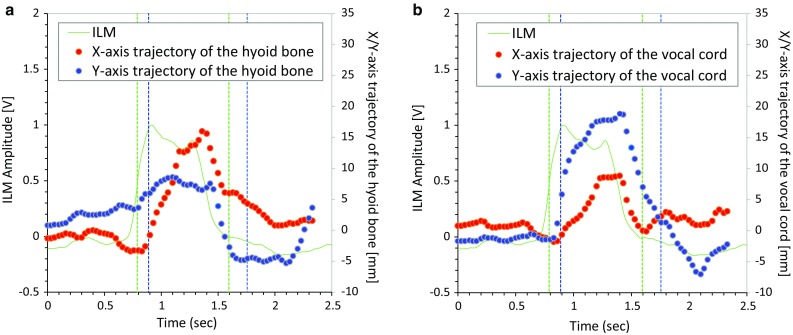
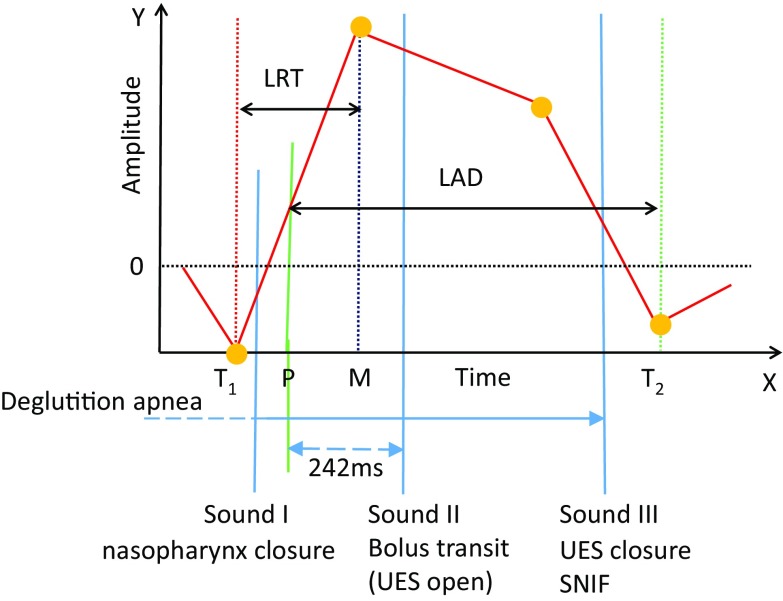
The assessment of swallowing function is important for the prevention of aspiration pneumonia. We developed a new swallowing monitoring system that uses respiratory flow, swallowing sound, and laryngeal motion. We applied this device to 11 healthy volunteers and 10 patients with dysphagia. Videofluoroscopy (VF) was conducted simultaneously with swallowing monitoring using our device. We measured laryngeal rising time (LRT), the time required for the larynx to elevate to the highest position, and laryngeal activation duration (LAD), the duration between the onset of rapid laryngeal elevation and the time when the larynx returned to the lowest position. In addition, we evaluated the coordination between swallowing and breathing. We found that LAD was correlated with a VF-derived parameter, pharyngeal response duration (PRD) in healthy subjects (LAD: 959 ± 259 ms vs. PRD: 1062 ± 149 ms, r = 0.60); however, this correlation was not found in the dysphagia patients. LRT was significantly prolonged in patients (healthy subjects: 320 ± 175 ms vs.
Patients: 465 ± 295 ms, P < 0.001, t test). Furthermore, frequency of swallowing immediately after inspiration was significantly increased in patients. Therefore, the new device may facilitate the assessment of some aspects of swallowing dysfunction.
Keywords: Coordination between swallowing and breathing; Deglutition apnea; Dysphagia; Swallowing.
Conflict of interest statement
This study has been conducted with funding support of Foodcare Co., Ltd. and J Craft Co., Ltd.
Figures

References
-
- Aboofazeli M, Moussavi Z. Automated classification of swallowing and breadth sounds. Conf Proc IEEE Eng Med Biol Soc. 2004;5:3816–3819. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
