

Is there an added value of faecal calprotectin and haemoglobin in the diagnostic work-up for primary care patients suspected of significant colorectal disease? A cross-sectional diagnostic study
- PMID: 27666114
- PMCID: PMC5036273
- DOI: 10.1186/s12916-016-0684-5
Is there an added value of faecal calprotectin and haemoglobin in the diagnostic work-up for primary care patients suspected of significant colorectal disease? A cross-sectional diagnostic study
Abstract
Background: The majority of primary care patients referred for bowel endoscopy do not have significant colorectal disease (SCD), and are - in hindsight - unnecessarily exposed to a small but realistic risk of severe endoscopy-associated complications. We developed a diagnostic strategy to better exclude SCD in these patients and evaluated the value of adding a faecal calprotectin point-of-care (POC) and/or a POC faecal immunochemical test for haemoglobin (FIT) to routine clinical information.
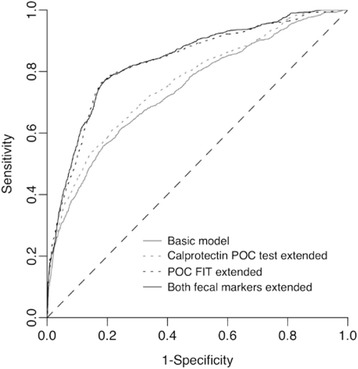
Methods: We used data from a prospective diagnostic study in SCD-suspected patients from 266 Dutch primary care practices referred for endoscopy to develop a diagnostic model for SCD with routine clinical information, which we extended with faecal calprotectin POC (quantitatively in μg/g faeces) and/or POC FIT results (qualitatively with a 6 μg/g faeces detection limit). We defined SCD as colorectal cancer (CRC), inflammatory bowel disease, diverticulitis, or advanced adenoma (>1 cm).
Results: Of 810 patients, 141 (17.4 %) had SCD. A diagnostic model with routine clinical data discriminated between patients with and without SCD with an area under the receiver operating characteristic curve (AUC) of 0.741 (95 % CI, 0.694-0.789). This AUC increased to 0.763 (95 % CI, 0.718-0.809; P = 0.078) when adding the calprotectin POC test, to 0.831 (95 % CI, 0.791-0.872; P < 0.001) when adding the POC FIT, and to 0.837 (95 % CI, 0.798-0.876; P < 0.001) upon combined extension. At a ≥ 5.0 % SCD probability threshold for endoscopy referral, 30.4 % of the patients tested negative based on this combined POC-tests extended model (95 % CI, 25.7-35.3 %), with 96.4 % negative predictive value (95 % CI, 93.1-98.2 %) and 93.7 % sensitivity (95 % CI, 88.2-96.8 %). Excluding the calprotectin POC test from this model still yielded 30.1 % test negatives (95 % CI, 24.7-35.6 %) and 96.0 % negative predictive value (95 % CI, 92.6-97.9 %), with 93.0 % sensitivity (95 % CI, 87.4-96.4 %).
Conclusions: FIT - and to a much lesser extent calprotectin - POC testing showed incremental value for SCD diagnosis beyond standard clinical information. A diagnostic strategy with routine clinical data and a POC FIT test may safely rule out SCD and prevent unnecessary endoscopy referral in approximately one third of SCD-suspected primary care patients. Please see related article: http://bmcmedicine.biomedcentral.com/articles/10.1186/s12916-016-0694-3 .
Figures

References
-
- Gonvers JJ, Harris JK, Wietlisbach V, et al. A European view of diagnostic yield and appropriateness of colonoscopy. Hepatogastroenterol. 2007;54:729–35. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
