

Elevated First-Trimester Total Bile Acid is Associated with the Risk of Subsequent Gestational Diabetes
- PMID: 27667090
- PMCID: PMC5036171
- DOI: 10.1038/srep34070
Elevated First-Trimester Total Bile Acid is Associated with the Risk of Subsequent Gestational Diabetes
Abstract
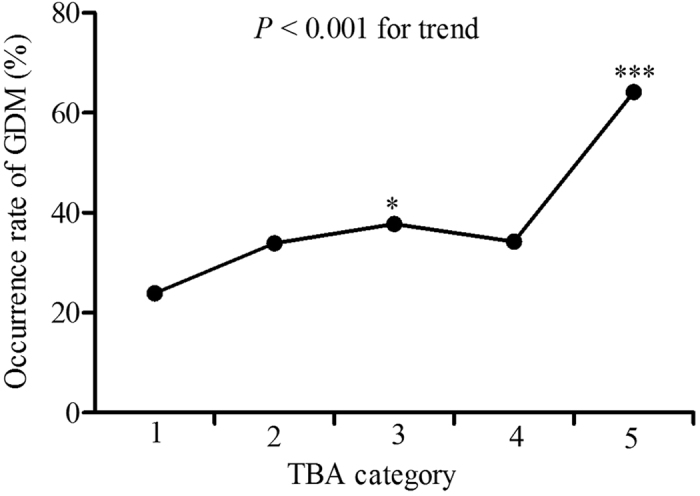
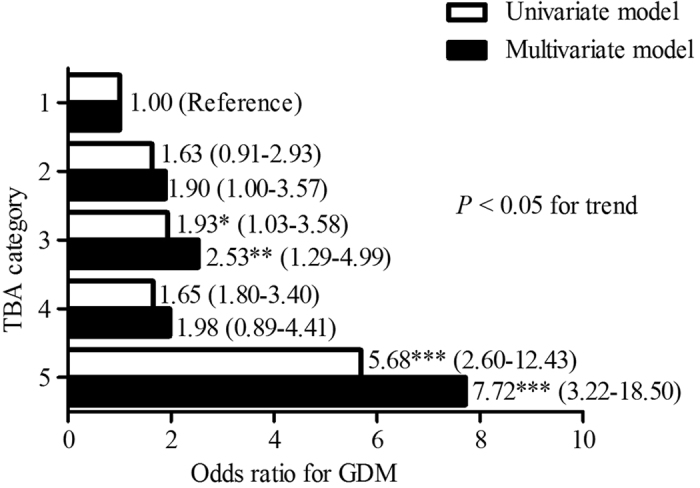
The aim of the current study is to assess whether total bile acid (TBA) level in first trimester pregnancy is associated with gestational diabetes mellitus (GDM). Biochemical parameters including serum TBA of 742 pregnant women were collected within 12 weeks of gestation and compared. At 24-28th weeks of gestation, 75 g oral glucose tolerance test (OGTT) was performed. The perinatal data of 330 women were collected. The results demonstrated women with GDM (n = 268) had higher first-trimester serum levels of TBA compared with healthy subjects (n = 474) (2.3 ± 1.4 μmol/L vs. 1.9 ± 1.0 μmol/L, P < 0.001). TBA was independently associated with GDM [adjusted odds ratio (AOR), 1.38; 95% confidence interval (CI), 1.18-1.61, P < 0.001]. Compared to the first category of TBA, women in the highest category had a marked increase in risk for GDM (AOR, 7.72; 95% CI, 3.22-18.50, P < 0.001). In conclusion, higher first-trimester TBA levels, even within normal range, may help indicate increased risk of GDM.
Figures
References
-
- Chang Y., Chen X., Cui H., Zhang Z. & Cheng L. Follow-up of postpartum women with gestational diabetes mellitus (GDM). Diabetes Res Clin Pract 106, 236–240 (2014). - PubMed
-
- Metzger B. E. et al.. Hyperglycemia and adverse pregnancy outcomes. N Engl J Med 358, 1991–2002 (2008). - PubMed
-
- Ryan E. A., O’Sullivan M. J. & Skyler J. S. Insulin action during pregnancy. Studies with the euglycemic clamp technique. Diabetes 34, 380–389 (1985). - PubMed
-
- Buchanan T. A., Xiang A., Kjos S. L. & Watanabe R. What is gestational diabetes? Diabetes care 30 Suppl 2, S105–S111 (2007). - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
