

Bronchial reacutization and gastroesophageal reflux: is there a potential clinical correlation?
- PMID: 27668224
- PMCID: PMC5009036
- DOI: 10.21037/atm.2016.08.40
Bronchial reacutization and gastroesophageal reflux: is there a potential clinical correlation?
Abstract
Background: Pepsin plays a role in gastroesophageal reflux (GER). Aims of this study were to verify if pepsin could be the cause of frequent bronchial exacerbations and to check if the persistence of chronic respiratory symptoms were correlated with pre-existing respiratory diseases.
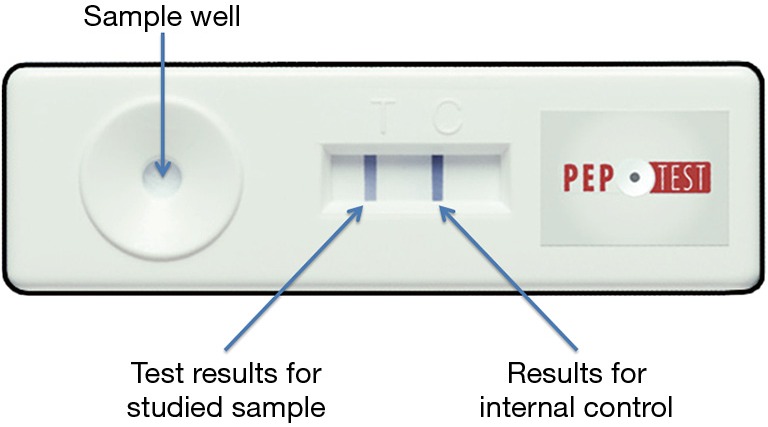
Methods: From January to May 2016, 42 patients underwent a diagnostic bronchoscopy. All patients had a history of at least one bronchial exacerbation during the previous year. Bronchial lavage fluid specimens were obtained. A semiquantitative assessment of pepsin in the samples was carried out based on the intensity of the test sample.
Results: Pepsin was present in 37 patients (88%), but in patients with bronchial asthma and chronic obstructive pulmonary disease (COPD), the finding of pepsin in the bronchoalveolar fluid was 100%. There was a strong positive statistical correlation between pepsin detection and radiological signs of GER (ρ=0.662), and between pepsin detection and diagnosis (ρ=0.682). No correlation was found between the bacteriology and the presence of pepsin in the airways (ρ=0.006).
Conclusions: The presence of pepsin in the airways shows the occurrence of reflux. The persistence of respiratory symptoms by at least 2 months suggest an endoscopic bronchial examination. This straightforward test confirms the cause possible irritation of the airways and may prevent further diagnostic tests, such as an EGD or pH monitoring esophageal.
Keywords: Bronchial reacutization; bronchoscopy; gastroesophageal reflux (GER); pepsin.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol 2006;101:1900-20; quiz 1943. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources