

A General Framework for Considering Selection Bias in EHR-Based Studies: What Data Are Observed and Why?
- PMID: 27668265
- PMCID: PMC5013936
- DOI: 10.13063/2327-9214.1203
A General Framework for Considering Selection Bias in EHR-Based Studies: What Data Are Observed and Why?
Abstract
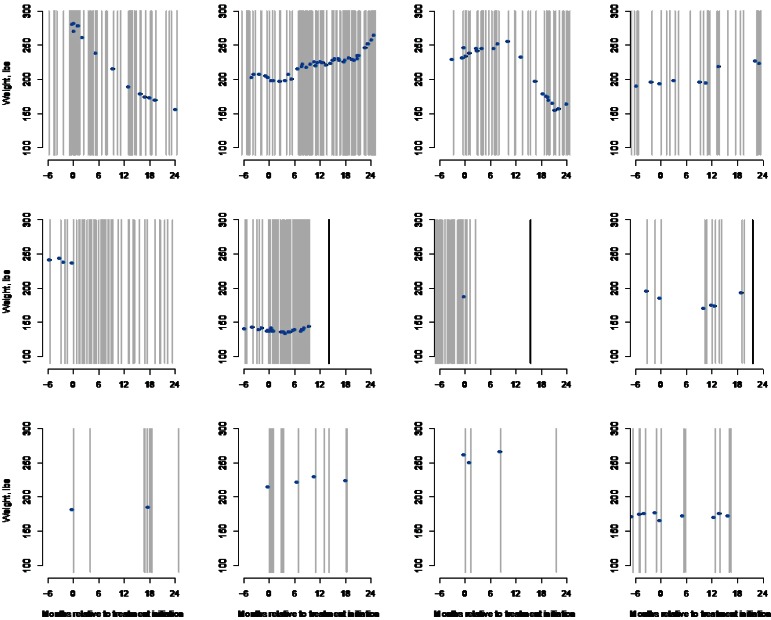
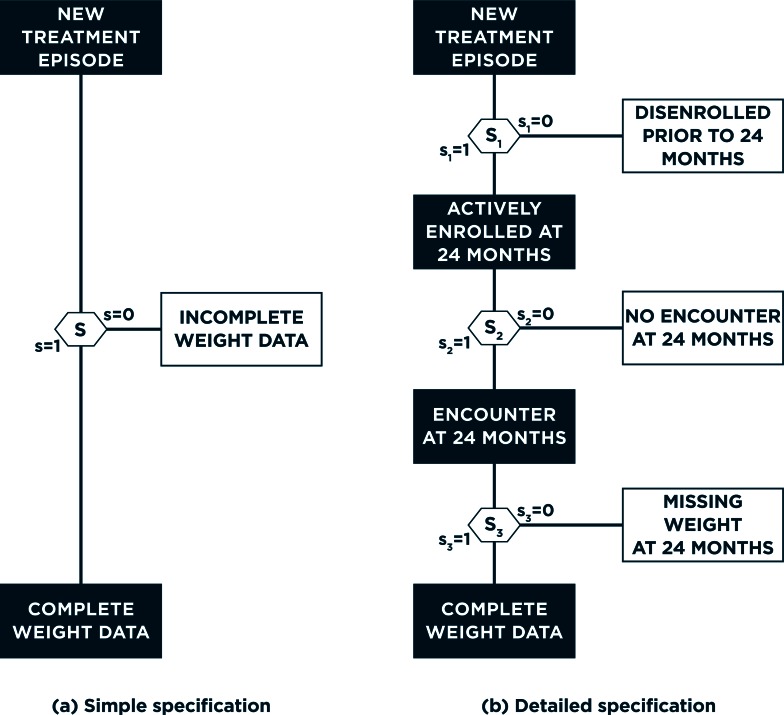
Electronic health records (EHR) data are increasingly seen as a resource for cost-effective comparative effectiveness research (CER). Since EHR data are collected primarily for clinical and/or billing purposes, their use for CER requires consideration of numerous methodologic challenges including the potential for confounding bias, due to a lack of randomization, and for selection bias, due to missing data. In contrast to the recent literature on confounding bias in EHR-based CER, virtually no attention has been paid to selection bias possibly due to the belief that standard methods for missing data can be readily-applied. Such methods, however, hinge on an overly simplistic view of the available/missing EHR data, so that their application in the EHR setting will often fail to completely control selection bias. Motivated by challenges we face in an on-going EHR-based comparative effectiveness study of choice of antidepressant treatment and long-term weight change, we propose a new general framework for selection bias in EHR-based CER. Crucially, the framework provides structure within which researchers can consider the complex interplay between numerous decisions, made by patients and health care providers, which give rise to health-related information being recorded in the EHR system, as well as the wide variability across EHR systems themselves. This, in turn, provides structure within which: (i) the transparency of assumptions regarding missing data can be enhanced, (ii) factors relevant to each decision can be elicited, and (iii) statistical methods can be better aligned with the complexity of the data.
Keywords: 2014 Group Health Seattle Symposium; Comparative Effectiveness Research (CER); Electronic Health Record (EHR); Methods; Missing Data; Selection Bias.
Figures

References
-
- Schneeweiss S, Avorn J. A review of uses of health care utilization databases for epidemiologic research on therapeutics. Journal of Clinical Epidemiology. 2005 Apr;58(4):323–337. - PubMed
-
- Weiner MG, Embi PJ. Toward reuse of clinical data for research and quality improvement: the end of the beginning? Annals of Internal Medicine. 2009 Sep 1;151(5):359–360. - PubMed
-
- Gallego B, Dunn AG, Coiera E. Role of electronic health records in comparative effectiveness research. J Comp Eff Res. 2013 Nov;2(6):529–532. - PubMed
-
- Institute of Medicine (US) Committee on Comparative Effectiveness Research Prioritization. Initial national priorities for comparative effectiveness research. Washington, D.C: National Academies Press; 2009.
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources