

How to design clinical rehabilitation trials for the upper paretic limb early post stroke?
- PMID: 27669893
- PMCID: PMC5037599
- DOI: 10.1186/s13063-016-1592-x
How to design clinical rehabilitation trials for the upper paretic limb early post stroke?
Abstract
Background: The impact of spontaneous neurobiological recovery is still neglected in designing rehabilitation trials early post stroke. We aimed to investigate the impact of the timing of randomization and prognostic stratification on the required sample sizes that are needed to reveal significant intervention effects on upper limb function at 26 weeks after first-ever ischemic stroke.
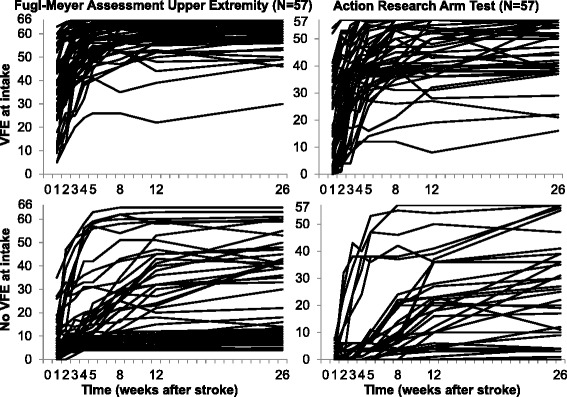
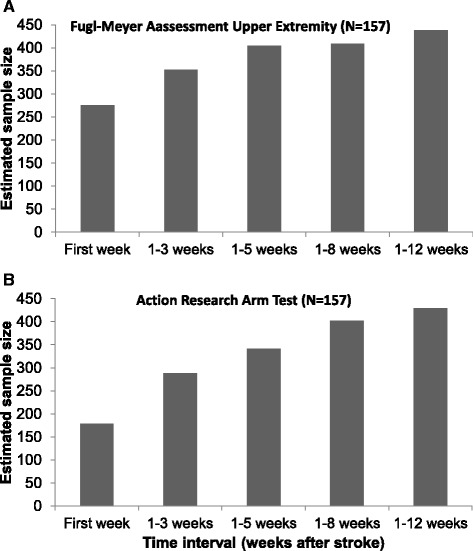
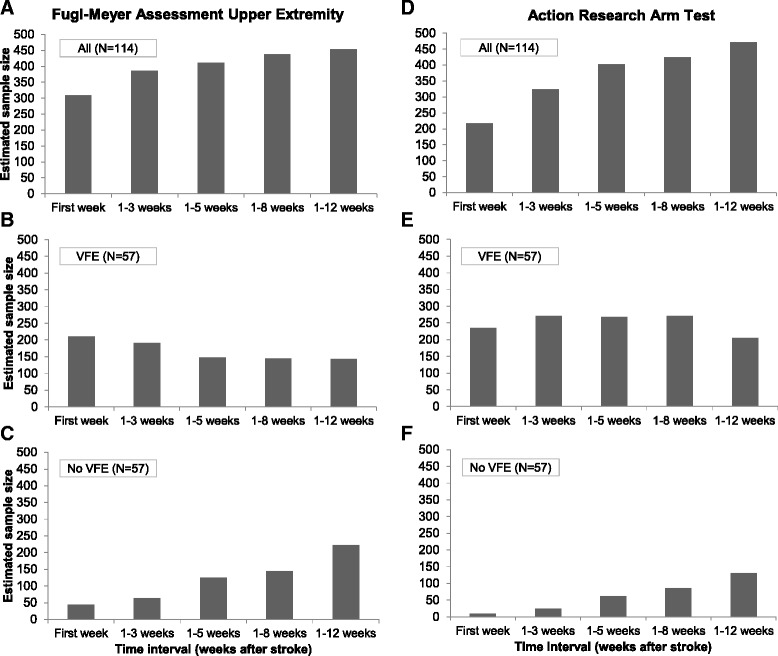
Method: Sample size calculations were based on a cohort study of 159 patients, using the Fugl-Meyer Assessment Upper Extremity and Action Research Arm Test as outcome measures (power = 80 %; two-tailed alpha = 0.05). We investigated different scenarios: random sampling of patients within five time intervals (stroke onset to 1, 3, 5, 8 and 12 weeks post stroke), and within stratified groups according to the presence or absence of voluntary extension of the thumb and/or two or more fingers at intake.
Results: The heterogeneity between outcome scores of patients, and subsequently the required sample sizes, increased from the first to the fifth time interval. Compared to the whole group, the sample sizes for both stratified groups (i.e., patients with and without Voluntary Finger Extension (VFE)) were lower. The required sample sizes for the patient group without VFE markedly increased when the time interval was broadened from 1 to 12 weeks post stroke, as opposed to the decrease seen for the group of patients with VFE.
Conclusion: These results are fundamental for designing upper limb trials early post stroke. To prevent type II error, future upper limb trials should randomize patients at a fixed moment early post stroke and stratify patients according to their potential neurobiological recovery.
Trial registration: Netherlands Trial Registry, www.trialregister.nl , NTR1424 , registered on 27 August 2008.
Keywords: Power; Prognostic stratification; Randomized controlled trial; Sample size; Stroke; Upper extremity.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
