

Enrichment of the lung microbiome with gut bacteria in sepsis and the acute respiratory distress syndrome
- PMID: 27670109
- PMCID: PMC5076472
- DOI: 10.1038/nmicrobiol.2016.113
Enrichment of the lung microbiome with gut bacteria in sepsis and the acute respiratory distress syndrome
Abstract
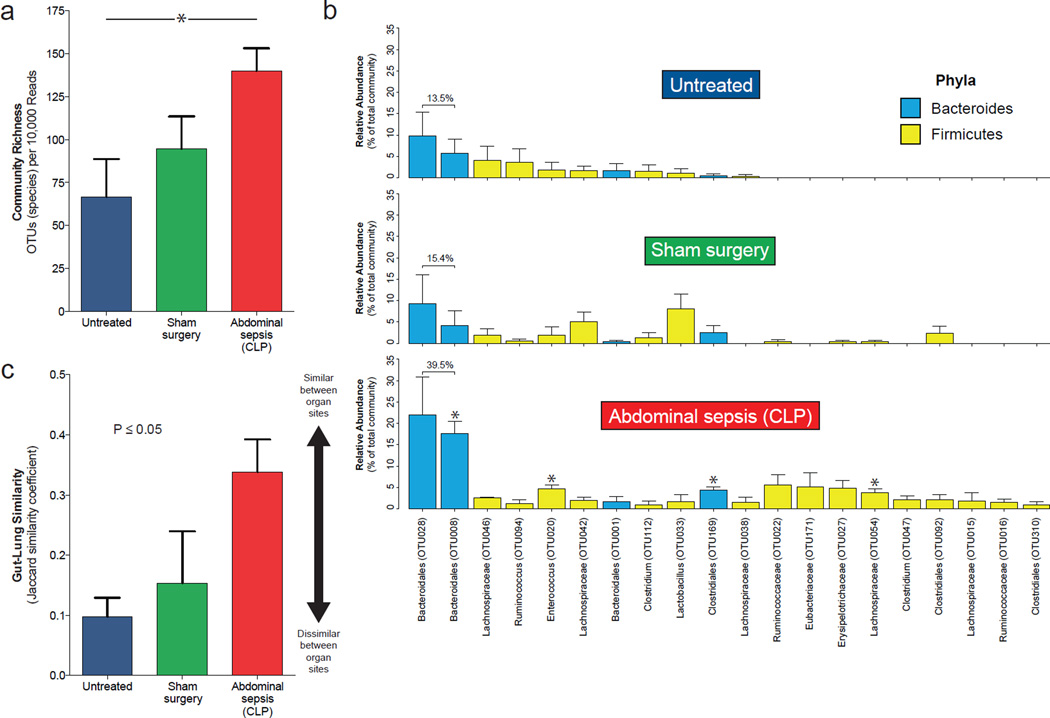
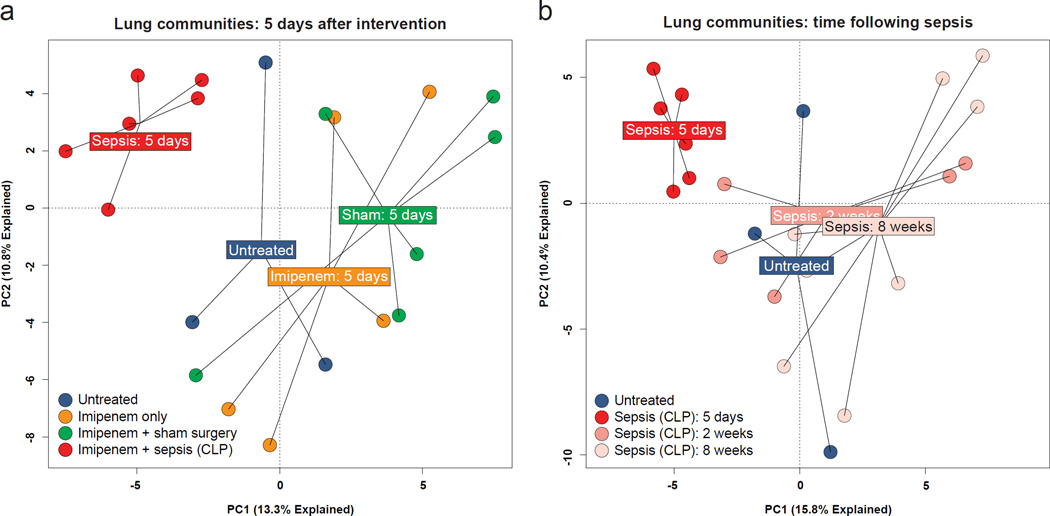
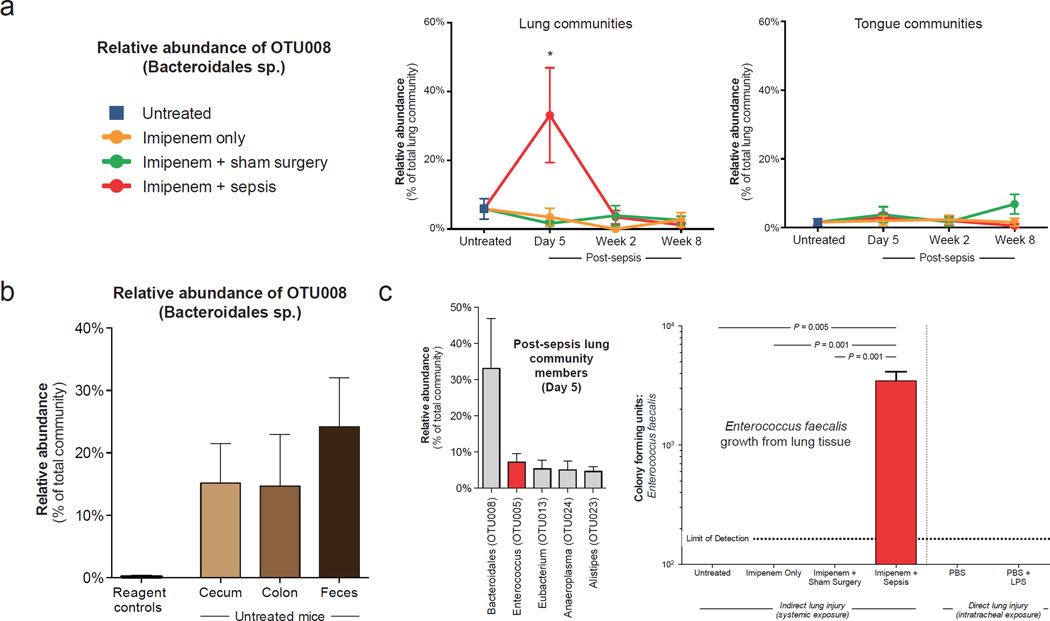
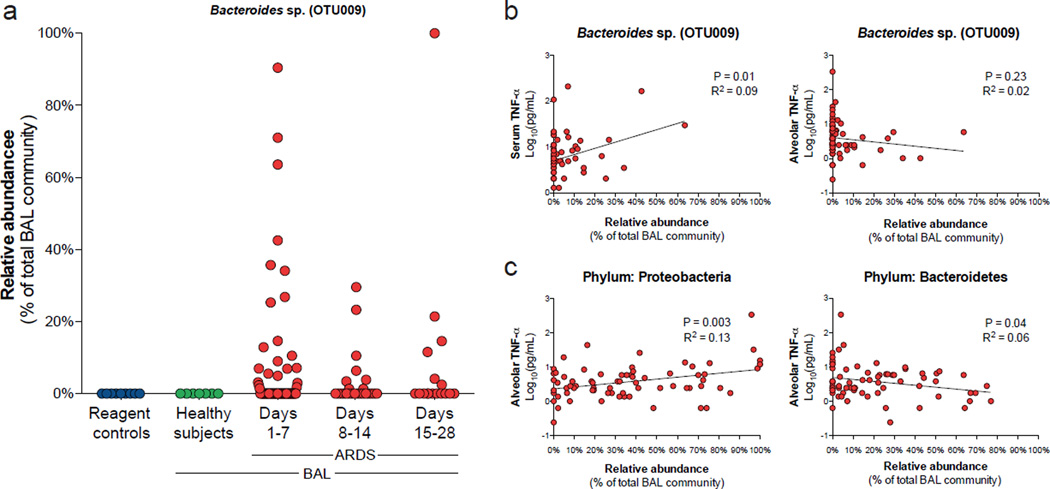
Sepsis and the acute respiratory distress syndrome (ARDS) are major causes of mortality without targeted therapies. Although many experimental and clinical observations have implicated gut microbiota in the pathogenesis of these diseases, culture-based studies have failed to demonstrate translocation of bacteria to the lungs in critically ill patients. Here, we report culture-independent evidence that the lung microbiome is enriched with gut bacteria both in a murine model of sepsis and in humans with established ARDS. Following experimental sepsis, lung communities were dominated by viable gut-associated bacteria. Ecological analysis identified the lower gastrointestinal tract, rather than the upper respiratory tract, as the likely source community of post-sepsis lung bacteria. In bronchoalveolar lavage fluid from humans with ARDS, gut-specific bacteria (Bacteroides spp.) were common and abundant, undetected by culture and correlated with the intensity of systemic inflammation. Alveolar TNF-α, a key mediator of alveolar inflammation in ARDS, was significantly correlated with altered lung microbiota. Our results demonstrate that the lung microbiome is enriched with gut-associated bacteria in sepsis and ARDS, potentially representing a shared mechanism of pathogenesis in these common and lethal diseases.
Figures
Comment in
-
Novel Discoveries and Advances in Management of Acute Respiratory Distress Syndrome.Am J Respir Crit Care Med. 2017 May 1;195(9):1264-1266. doi: 10.1164/rccm.201612-2478RR. Am J Respir Crit Care Med. 2017. PMID: 28288286 No abstract available.
References
-
- Angus DC, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit. Care Med. 2001;29:1303–1310. - PubMed
-
- Rubenfeld GD, et al. Incidence and outcomes of acute lung injury. N. Engl. J. Med. 2005;353:1685–1693. - PubMed
-
- Hudson LD, Milberg JA, Anardi D, Maunder RJ. Clinical risks for development of the acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1995;151:293–301. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
