

Physiological and molecular responses to bariatric surgery: markers or mechanisms underlying T2DM resolution?
- PMID: 27671525
- PMCID: PMC9190117
- DOI: 10.1111/nyas.13194
Physiological and molecular responses to bariatric surgery: markers or mechanisms underlying T2DM resolution?
Abstract
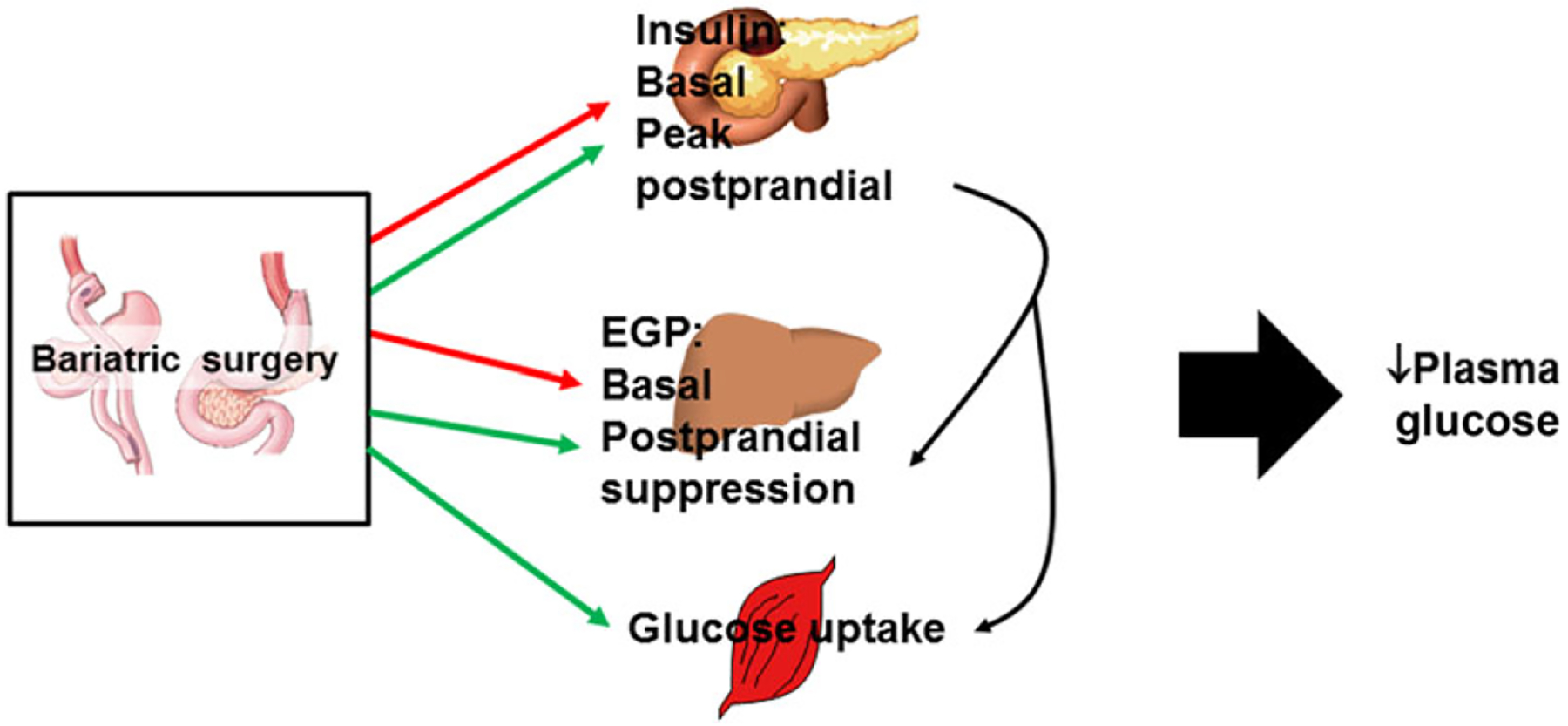
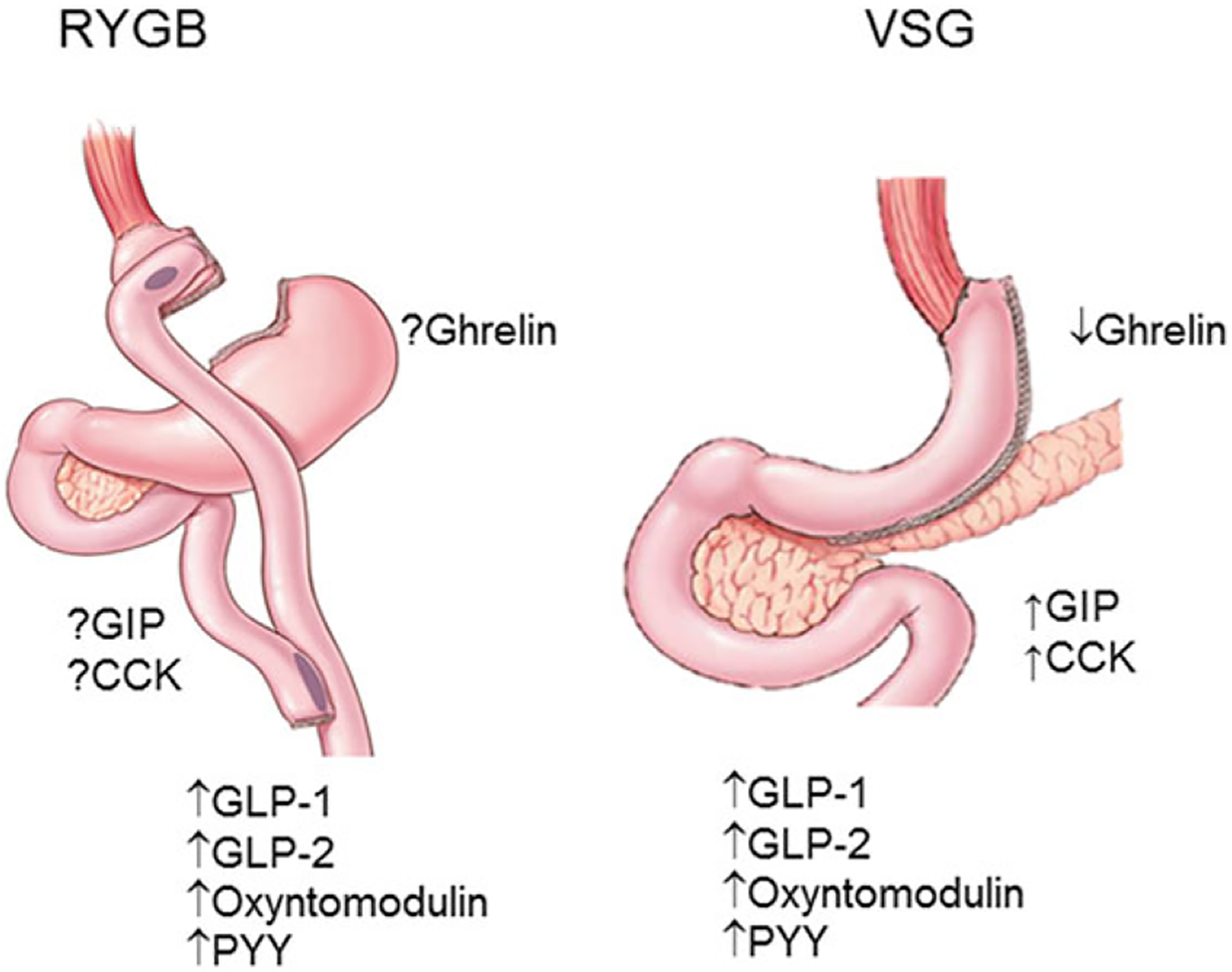
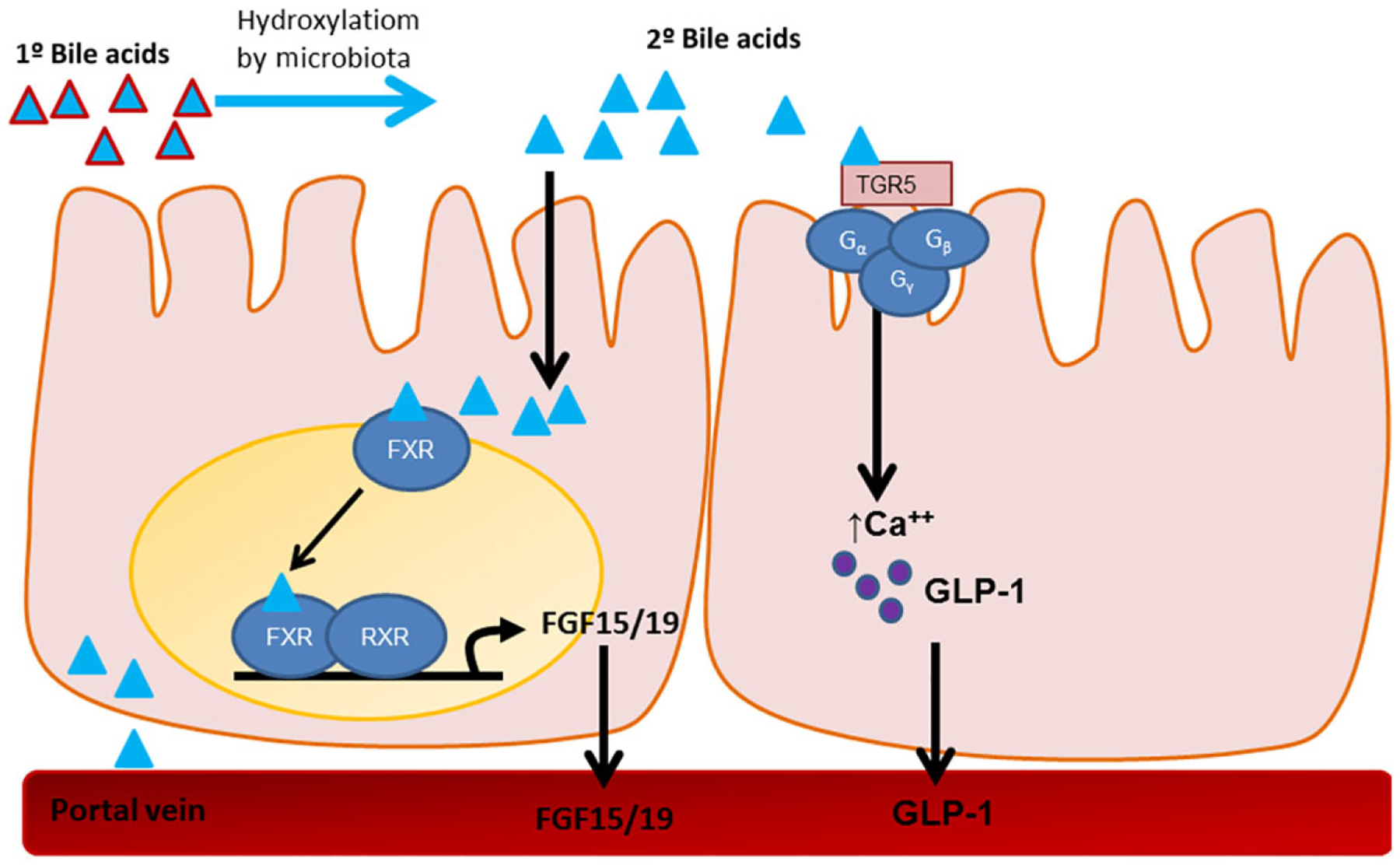
Bariatric surgery is currently the most effective treatment for obesity and associated comorbidities, including rapid resolution of type 2 diabetes mellitus (T2DM). Although the weight loss itself has substantial impact, bariatric surgery also has weight loss-independent effects on T2DM. Several variations of bariatric surgery exist, including the widely studied Roux-en-Y gastric bypass and vertical sleeve gastrectomy. The success of both of these bariatric surgeries was originally attributed to restrictive and malabsorptive modes of action; however, mounting evidence from both human and animal studies implicates mechanisms beyond surgery-induced mechanical changes to the gastrointestinal (GI) system. In fact, with bariatric surgery comes a spectrum of physiological responses, including postprandial enhancement of gut peptide and bile acids levels, restructuring of microbial composition, and changes in GI function and morphology. Although many of these processes are also essential for glucoregulation, the independent role of each in the success of surgery is still an open question. In this review, we explore whether these changes are necessary for the improvements in body mass and glucose homeostasis or whether they are simply markers of the physiological effect of surgery.
Keywords: bariatric surgery; glucose metabolism; type 2 diabetes.
© 2016 New York Academy of Sciences.
Figures
References
-
- Makary MA et al. 2010. Medication utilization and annual health care costs in patients with type 2 diabetes mellitus before and after bariatric surgery. Arch. Surg 145: 726–731. - PubMed
-
- Sjöström L et al. 2007. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med 357: 741–752. - PubMed
-
- Adams TD et al. 2007. Long-term mortality after gastric bypass surgery. N. Engl. J. Med 357: 753–761. - PubMed
-
- Pontiroli AE & Morabito A. 2011. Long-term prevention of mortality in morbid obesity through bariatric surgery. A systematic review and meta-analysis of trials performed with gastric banding and gastric bypass. Ann. Surg 253: 484–487. - PubMed
-
- Ashrafian H et al. 2011. Metabolic surgery and cancer: protective effects of bariatric procedures. Cancer 117: 1788–1799. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
