

Split liver transplantation in adults
- PMID: 27672272
- PMCID: PMC5011665
- DOI: 10.3748/wjg.v22.i33.7500
Split liver transplantation in adults
Abstract
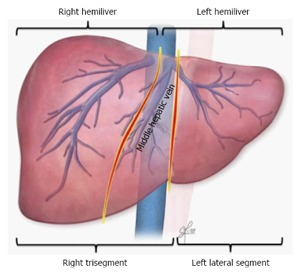
Split liver transplantation (SLT), while widely accepted in pediatrics, remains underutilized in adults. Advancements in surgical techniques and donor-recipient matching, however, have allowed expansion of SLT from utilization of the right trisegment graft to now include use of the hemiliver graft as well. Despite less favorable outcomes in the early experience, better outcomes have been reported by experienced centers and have further validated the feasibility of SLT. Importantly, more than two decades of experience have identified key requirements for successful SLT in adults. When these requirements are met, SLT can achieve outcomes equivalent to those achieved with other types of liver transplantation for adults. However, substantial challenges, such as surgical techniques, logistics, and ethics, persist as ongoing barriers to further expansion of this highly complex procedure. This review outlines the current state of SLT in adults, focusing on donor and recipient selection based on physiology, surgical techniques, surgical outcomes, and ethical issues.
Keywords: Adults; Donor and recipient selection; Ethical issues; Graft size; Graft survival; Split liver transplantation; Surgical technique.
Conflict of interest statement
Conflict-of-interest statement: The authors declare no conflicts of interest or potential conflicts of interest for this article.
Figures

References
-
- Bismuth H, Houssin D. Reduced-sized orthotopic liver graft in hepatic transplantation in children. Surgery. 1984;95:367–370. - PubMed
-
- Pichlmayr R, Ringe B, Gubernatis G, Hauss J, Bunzendahl H. [Transplantation of a donor liver to 2 recipients (splitting transplantation)--a new method in the further development of segmental liver transplantation] Langenbecks Arch Chir. 1988;373:127–130. - PubMed
-
- Bismuth H, Morino M, Castaing D, Gillon MC, Descorps Declere A, Saliba F, Samuel D. Emergency orthotopic liver transplantation in two patients using one donor liver. Br J Surg. 1989;76:722–724. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
