

Hepatobiliary and pancreatic ascariasis
- PMID: 27672273
- PMCID: PMC5011666
- DOI: 10.3748/wjg.v22.i33.7507
Hepatobiliary and pancreatic ascariasis
Abstract
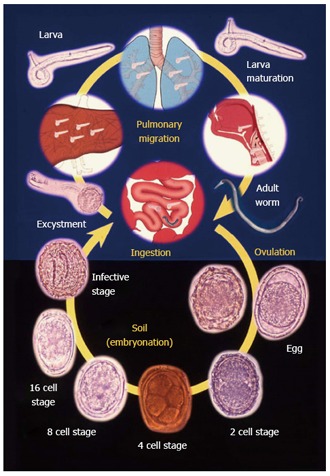
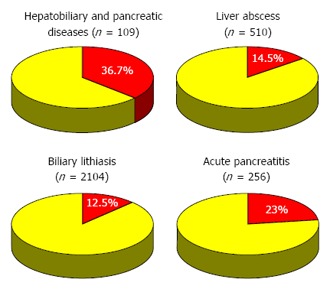
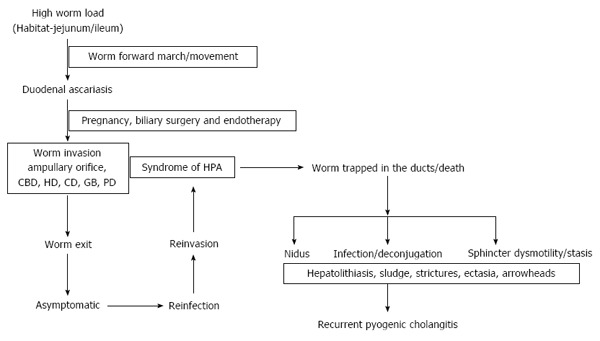
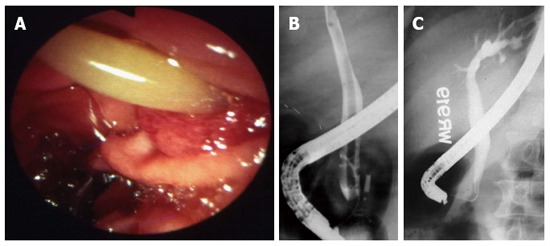
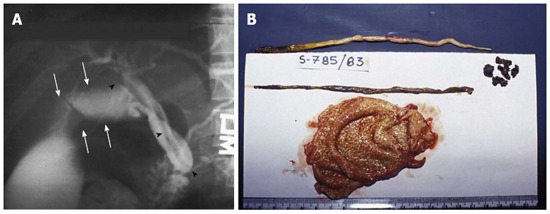
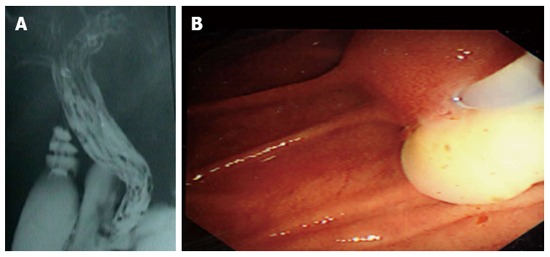
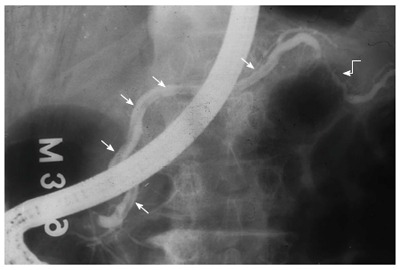
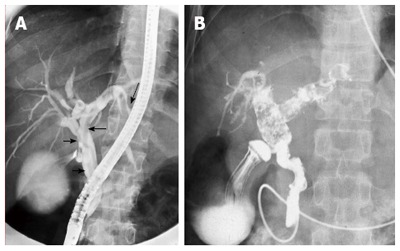
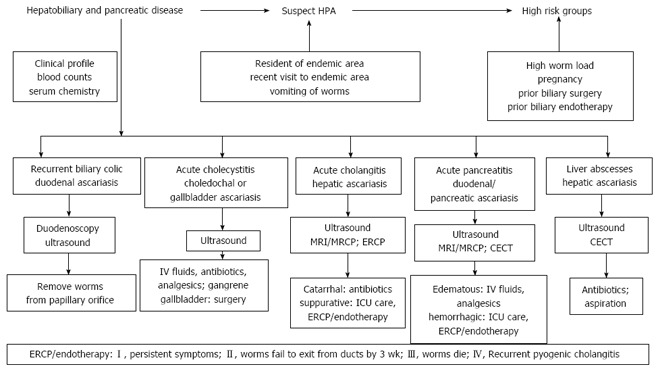
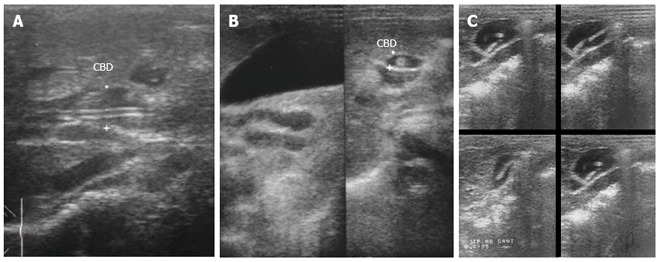
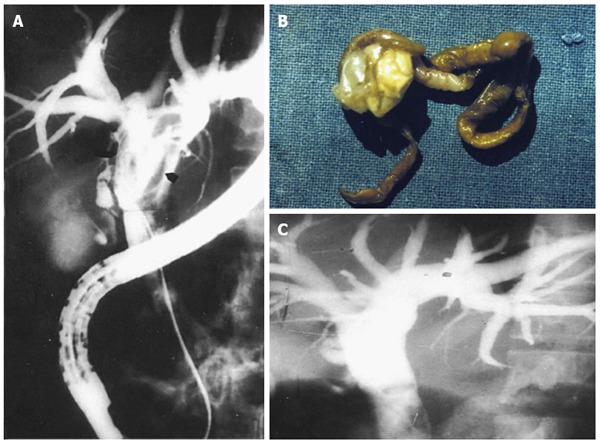
Hepatobiliary and pancreatic ascariasis (HPA) was described as a clinical entity from Kashmir, India in 1985. HPA is caused by invasion and migration of nematode, Ascaris lumbricoides, in to the biliary tract and pancreatic duct. Patients present with biliary colic, cholangitis, cholecystitis, hepatic abscesses and acute pancreatitis. Ascarides traverse the ducts repeatedly, get trapped and die, leading to formation of hepatolithiasis. HPA is ubiquitous in endemic regions and in Kashmir, one such region, HPA is the etiological factor for 36.7%, 23%, 14.5% and 12.5% of all biliary diseases, acute pancreatitis, liver abscesses and biliary lithiasis respectively. Ultrasonography is an excellent diagnostic tool in visualizing worms in gut lumen and ductal system. The rational treatment for HPA is to give appropriate treatment for clinical syndromes along with effective anthelmintic therapy. Endotherapy in HPA is indicated if patients continue to have symptoms on medical therapy or when worms do not move out of ductal lumen by 3 wk or die within the ducts. The worms can be removed from the ductal system in most of the patients and such patients get regression of symptoms of hepatobiliary and pancreatic disease.
Keywords: Ascaris lumbricoides; Biliary calculi; Cholangitis; Cholecystitis; Pancreatitis; Recurrent pyogenic cholangitis.
Conflict of interest statement
Conflict-of-interest statement: The authors report no conflict of interest.
Figures



References
-
- Khuroo MS, Zargar SA. Biliary ascariasis. A common cause of biliary and pancreatic disease in an endemic area. Gastroenterology. 1985;88:418–423. - PubMed
-
- Khuroo MS, Zargar SA, Mahajan R. Hepatobiliary and pancreatic ascariasis in India. Lancet. 1990;335:1503–1506. - PubMed
-
- Khuroo MS, Dar MY, Yattoo GN, Khan BA, Boda MI, Zargar SA, Javid G, Allai MS. Serial cholangiographic appearances in recurrent pyogenic cholangitis. Gastrointest Endosc. 1993;39:674–679. - PubMed
-
- Khuroo MS, Khuroo NS, Khuroo MS. Biliary ascariasis in the etiology of recurrent pyogenic cholangitis in an endemic area. International Journal of Hepatobiliary and Pancreatic Diseases. 2015;5:22.
-
- Khuroo MS. Ascariasis. Gastroenterol Clin North Am. 1996;25:553–577. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
