

New insights into the pathophysiology of achalasia and implications for future treatment
- PMID: 27672286
- PMCID: PMC5028805
- DOI: 10.3748/wjg.v22.i35.7892
New insights into the pathophysiology of achalasia and implications for future treatment
Abstract
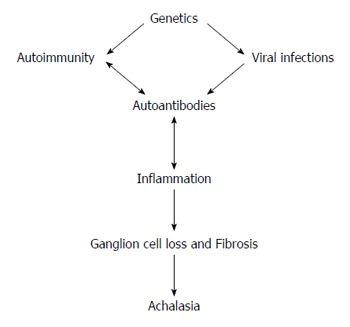
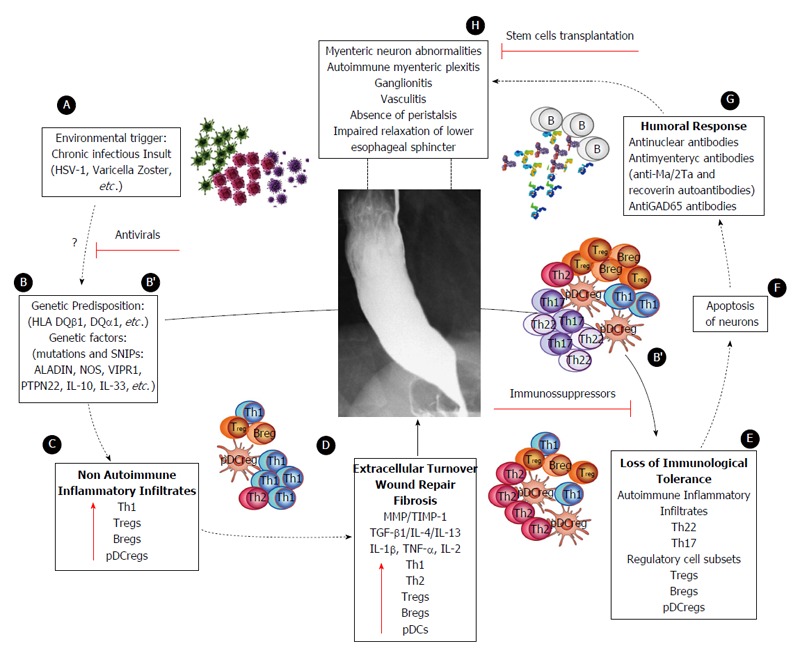
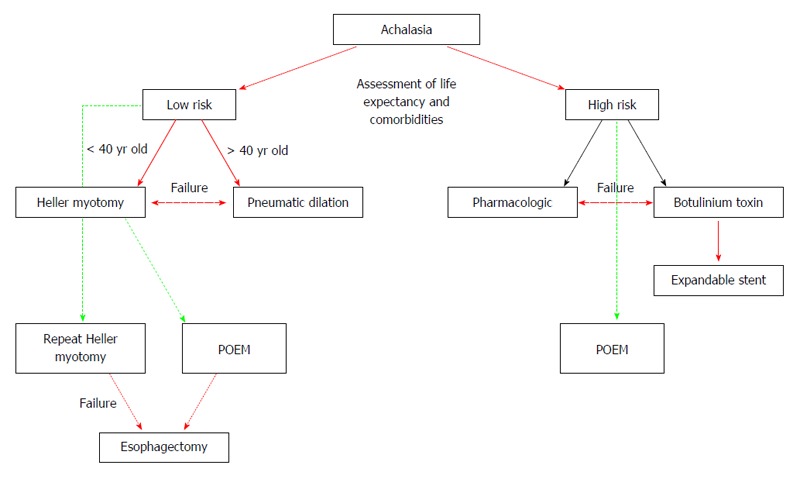
Idiopathic achalasia is an archetype esophageal motor disorder, causing significant impairment of eating ability and reducing quality of life. The pathophysiological underpinnings of this condition are loss of esophageal peristalsis and insufficient relaxation of the lower esophageal sphincter (LES). The clinical manifestations include dysphagia for both solids and liquids, regurgitation of esophageal contents, retrosternal chest pain, cough, aspiration, weight loss and heartburn. Even though idiopathic achalasia was first described more than 300 years ago, researchers are only now beginning to unravel its complex etiology and molecular pathology. The most recent findings indicate an autoimmune component, as suggested by the presence of circulating anti-myenteric plexus autoantibodies, and a genetic predisposition, as suggested by observed correlations with other well-defined genetic syndromes such as Allgrove syndrome and multiple endocrine neoplasia type 2 B syndrome. Viral agents (herpes, varicella zoster) have also been proposed as causative and promoting factors. Unfortunately, the therapeutic approaches available today do not resolve the causes of the disease, and only target the consequential changes to the involved tissues, such as destruction of the LES, rather than restoring or modifying the underlying pathology. New therapies should aim to stop the disease at early stages, thereby preventing the consequential changes from developing and inhibiting permanent damage. This review focuses on the known characteristics of idiopathic achalasia that will help promote understanding its pathogenesis and improve therapeutic management to positively impact the patient's quality of life.
Keywords: Achalasia; Autoimmune disease; Pathophysiology; Treatment.
Conflict of interest statement
Conflict-of-interest statement: The authors report no conflicts of interest.
Figures
References
-
- Sadowski DC, Ackah F, Jiang B, Svenson LW. Achalasia: incidence, prevalence and survival. A population-based study. Neurogastroenterol Motil. 2010;22:e256–e261. - PubMed
-
- Vaezi MF, Pandolfino JE, Vela MF. ACG clinical guideline: diagnosis and management of achalasia. Am J Gastroenterol. 2013;108:1238–149; quiz 1250. - PubMed
-
- Gockel I, Bohl JR, Doostkam S, Eckardt VF, Junginger T. Spectrum of histopathologic findings in patients with achalasia reflects different etiologies. J Gastroenterol Hepatol. 2006;21:727–733. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
