

Portal biliopathy
- PMID: 27672292
- PMCID: PMC5028811
- DOI: 10.3748/wjg.v22.i35.7973
Portal biliopathy
Abstract
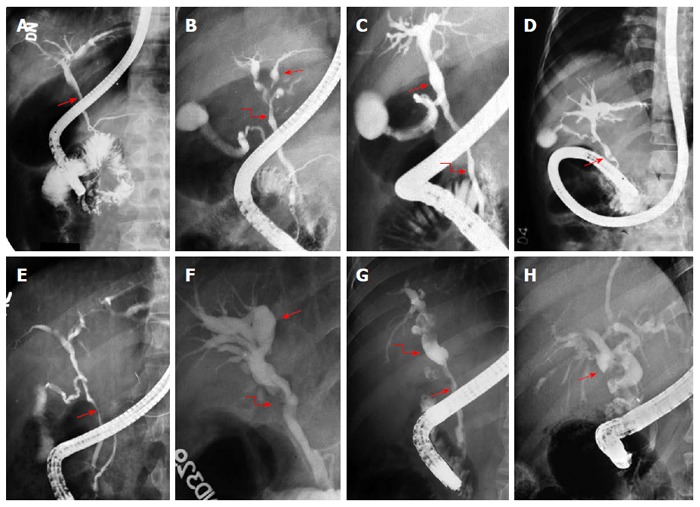
Portal biliopathy refers to cholangiographic abnormalities which occur in patients with portal cavernoma. These changes occur as a result of pressure on bile ducts from bridging tortuous paracholedochal, epicholedochal and cholecystic veins. Bile duct ischemia may occur due prolonged venous pressure effect or result from insufficient blood supply. In addition, encasement of ducts may occur due fibrotic cavernoma. Majority of patients are asymptomatic. Portal biliopathy is a progressive disease and patients who have long standing disease and more severe bile duct abnormalities present with recurrent episodes of biliary pain, cholangitis and cholestasis. Serum chemistry, ultrasound with color Doppler imaging, magnetic resonance imaging with magnetic resonance cholangiopancreatography and magnetic resonance portovenography are modalities of choice for evaluation of portal biliopathy. Endoscopic retrograde cholangiography being an invasive procedure is indicated for endotherapy only. Management of portal biliopathy is done in a stepwise manner. First, endotherapy is done for dilation of biliary strictures, placement of biliary stents to facilitate drainage and removal of bile duct calculi. Next portal venous pressure is reduced by formation of surgical porto-systemic shunt or transjugular intrahepatic portosystemic shunt. This causes significant resolution of biliary changes. Patients who persist with biliary symptoms and bile duct changes may benefit from surgical biliary drainage procedures (hepaticojejunostomy or choledechoduodenostomy).
Keywords: Bile duct calculi; Bile duct strictures; Biliary disease; Extrahepatic portal venous obstruction; Portal cavernoma.
Conflict of interest statement
Conflict-of-interest statement: The authors report no conflict of interest.
Figures






References
-
- Khuroo MS, Yattoo GN, Zargar SA, Javid G, Dar MY, Khan BA, Boda MI. Biliary abnormalities associated with extrahepatic portal venous obstruction. Hepatology. 1993;17:807–813. - PubMed
-
- Chandra R, Kapoor D, Tharakan A, Chaudhary A, Sarin SK. Portal biliopathy. J Gastroenterol Hepatol. 2001;16:1086–1092. - PubMed
-
- Khuroo MS. Landmarks in research-The Untold Stories: Portal Biliopathy-the biliary disease in extrahepatic portal hypertension. Available from: https://wwwresearchgatenet/publication/297916019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
