

Therapeutic hypothermia translates from ancient history in to practice
- PMID: 27673420
- PMCID: PMC5233584
- DOI: 10.1038/pr.2016.198
Therapeutic hypothermia translates from ancient history in to practice
Abstract
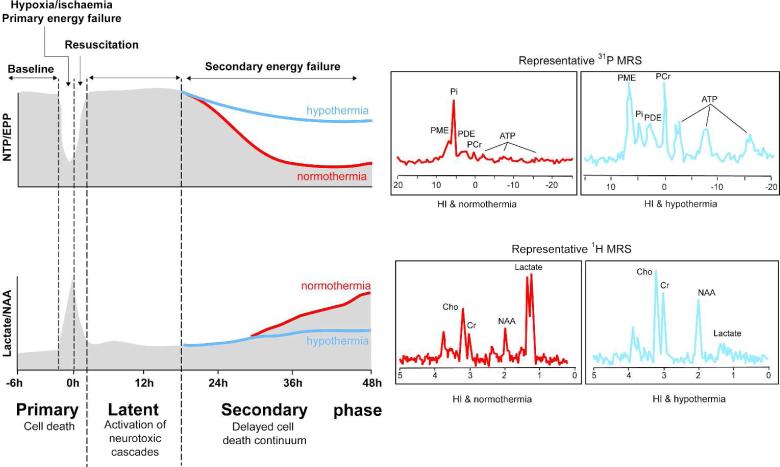
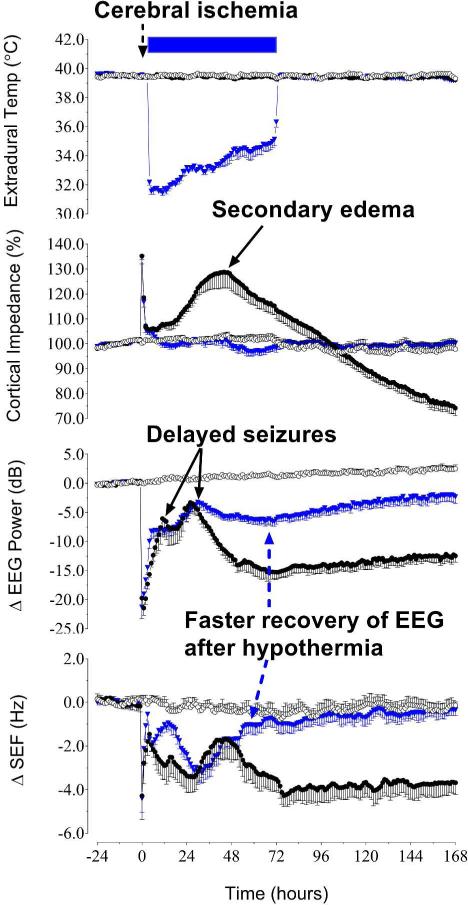
Acute postasphyxial encephalopathy around the time of birth remains a major cause of death and disability. The possibility that hypothermia may be able to prevent or lessen asphyxial brain injury is a "dream revisited". In this review, a historical perspective is provided from the first reported use of therapeutic hypothermia for brain injuries in antiquity, to the present day. The first uncontrolled trials of cooling for resuscitation were reported more than 50 y ago. The seminal insight that led to the modern revival of studies of neuroprotection was that after profound asphyxia, many brain cells show initial recovery from the insult during a short "latent" phase, typically lasting ~6 h, only to die hours to days later during a "secondary" deterioration phase characterized by seizures, cytotoxic edema, and progressive failure of cerebral oxidative metabolism. Studies designed around this conceptual framework showed that mild hypothermia initiated as early as possible before the onset of secondary deterioration, and continued for a sufficient duration to allow the secondary deterioration to resolve, is associated with potent, long-lasting neuroprotection. There is now compelling evidence from randomized controlled trials that mild induced hypothermia significantly improves intact survival and neurodevelopmental outcomes to midchildhood.
Figures
References
-
- Floyer J. An essay to restore the dipping of infants in their baptism; with a dialogue betwixt a curate and a practitioner, concerning the manner of immersion. Vol. 1722. Holland, London: p. 79.
-
- Celcus AC. On Medicine, Books 1-4. 1-100 AD. Harvard University Press, Loeb Classical Library; pp. 1–512.
-
- Hippocrates De Vetere Medicina. 460–375 BC. Harvard University Press, Loeb Classical Library; pp. 1–432.
-
- Edwards WF. Philadelphia, Haswell, Barrington and Haswell, London: 1832. On the Influence of Physical Agents on Life. pp. 1–489.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
