

Imaging Surveillance After Proximal Aortic Operations: Is it Necessary?
- PMID: 27677566
- PMCID: PMC5319874
- DOI: 10.1016/j.athoracsur.2016.06.085
Imaging Surveillance After Proximal Aortic Operations: Is it Necessary?
Abstract
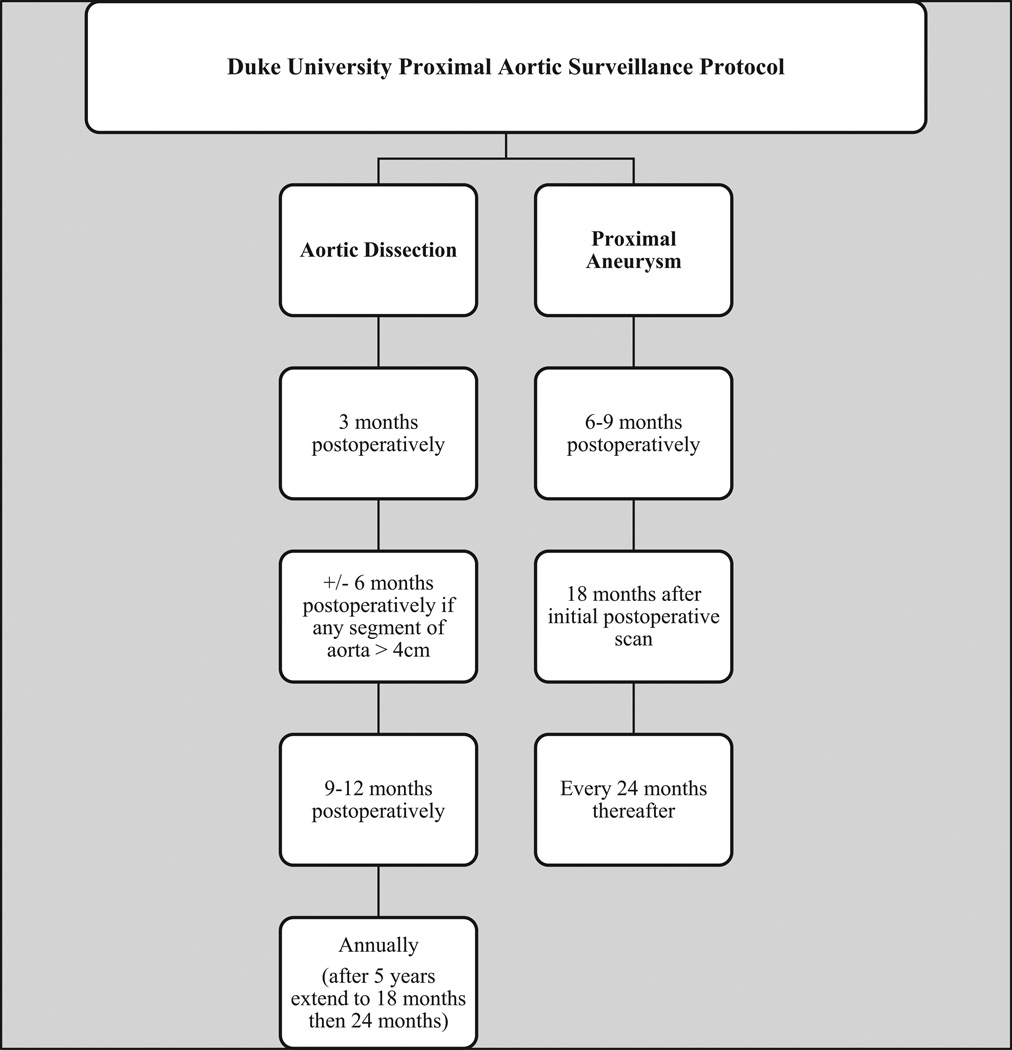
Background: Current guidelines for imaging surveillance after proximal aortic repair are not evidence based. This study sought to characterize the incidence and causes of reintervention after proximal aortic operations to provide data to guide the frequency and duration of postoperative surveillance.
Methods: Data on all patients undergoing proximal aortic operations (ascending, with or without root, with or without aortic valve replacement, or with or without arch) during a 9-year period (n = 869) at a single institution were prospectively collected. Patients who required reintervention on the proximal or distal aorta were identified and causes for reintervention determined. Planned two-stage repairs and index procedures done at other hospitals were excluded. The primary end point was the time to the first reintervention, and competing-risk Cox regression was used to model reintervention risk.
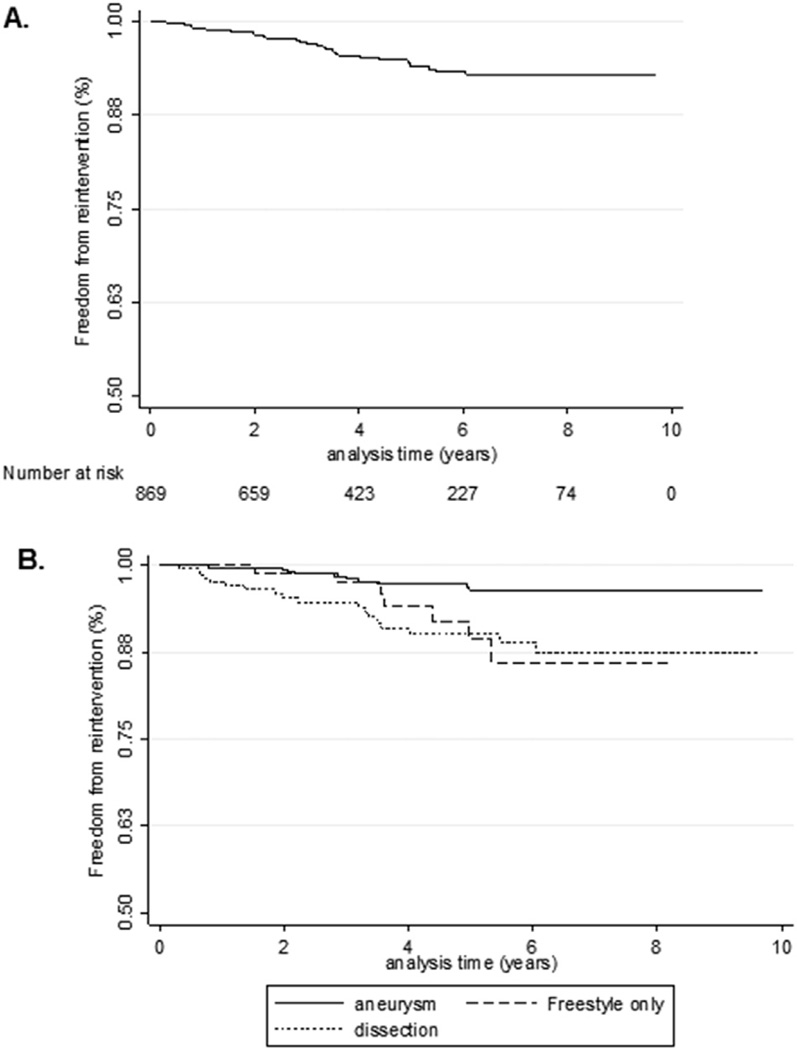
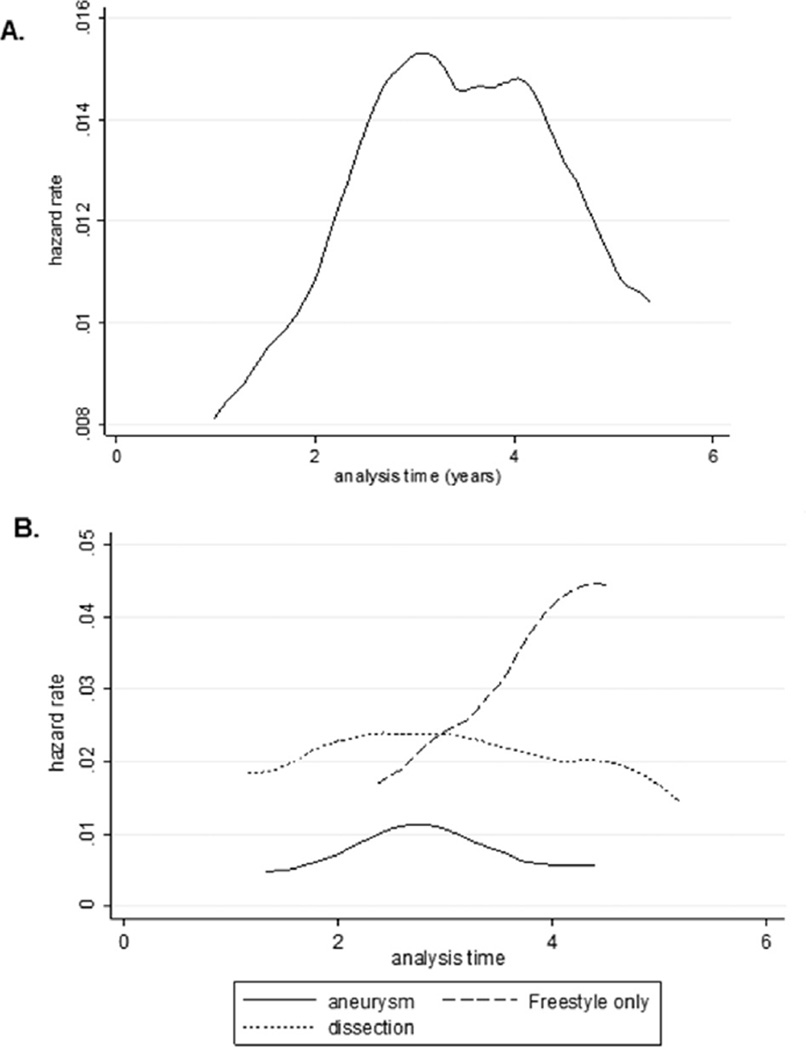
Results: Reinterventions occurred in 4.3% of patients (n = 37), with 48.6% (n = 18) involving the proximal aorta and 51.4% (n = 19) the distal. Median time to reintervention was 2.8 years (interquartile range, 1.5 to 3.6 years). For index aneurysm cases, reintervention for aneurysm of the descending/thoracoabdominal aorta and root were most common. Of the 6 root aneurysms/pseudoaneurysms, 5 (83%) were due to degeneration of a stentless porcine aortic root. For index type A dissections, reintervention for aneurysm of the descending/thoracoabdominal aorta and arch were most common. The mean duration of follow up was 4.2 ± 2.5 years. The 9-year actuarial freedom from reintervention was 92.9%. Cox regression showed index type A dissection was a significant predictor of time to aortic reintervention (hazard ratio, 2.01; 95% confidence interval, 1.04 to 3.9; p = 0.038).
Conclusions: Reinterventions after proximal aortic operations are uncommon; most occur within 3 years of the index operation and involve the proximal and distal aorta nearly equally. Patients with type A dissection or stentless porcine roots require aggressive surveillance, whereas a more liberal approach is suitable for patients without such risk factors. This strategy may reduce the lifetime radiation burden and health care costs.
Copyright © 2017 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Di Bartolomeo R, Berretta P, Petridis FD, et al. Reoperative surgery on the thoracic aorta. J Thorac Cardiovasc Surg. 2013;145:S78–S84. - PubMed
-
- Estrera AL, Miller CC, 3rd, Porat E, et al. Determinants of early and late outcome for reoperations of the proximal aorta. Ann Thorac Surg. 2004;78:837–845. - PubMed
-
- Etz CD, Plestis KA, Homann TM, et al. Reoperative aortic root and transverse arch procedures: a comparison with contemporaneous primary operations. J Thorac Cardiovasc Surg. 2008;136:860–867. - PubMed
-
- Fukunaga N, Koyama T, Konishi Y, Murashita T, Kanemitsu H, Okada Y. Clinical outcome of redo operation on aortic root. Gen Thorac Cardiovasc Surg. 2014;62:215–220. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
